Introduction
As per literature, primary duodenal squamous cell carcinoma is extremely rare; so far, only as few as 22 cases were reported. The median age of presentation was 63.78 years, predominantly in males.1 In general, the occurrence of malignancies in the small intestinal tract is very low, accounting for 0.1-1.3% 2 of all the gastrointestinal malignancies, whether metastatic or primary. The metastases in the gastrointestinal tract are rarely reported, such as from tumors from the lung, breast, liver, melanoma, testicular seminoma, choriocarcinoma, merkel cell carcinoma, malignant fibrous histiocytoma, and a few others.3, 4, 5, 6 Occurrence of metastatic squamous cell carcinoma involving the gastrointestinal tract occurring from primary lung tumors is also extremely rare. Occasional cases of gastric or duodenal involvement reported in the literature. 7, 8
Case Report
A 55-year-old male patient was presented to the gastroenterology department with anorexia, epigastric pain, and loss of weight, weakness, and vomiting. Laboratory investigation revealed abnormal LFT with elevated alkaline phosphates and GGT with normal bilirubin levels.
The patient was investigated with a PET-CT scan, which revealed metabolically active circumferential wall thickening involving the D2 segment of the duodenum with gastric outlet syndrome. No regional lymphadenopathy noted. No other metabolically active lesions noted in the rest of the body.
So the patient underwent the Whipple procedure (pancreatoduodenectomy).
On gross examination, a circumferential solid to friable whitish tumor in the D2 segment was noted. The tumor was seen limited to the duodenal lumen and invading up to the duodenal muscularis propria. The underlying pancreas was uninvolved.
On histopathology, the duodenal epithelium is ulcerated with subepithelial infiltration of tumor cells in clusters, nests, trabeculae, and sheets. The individual cells are polygonal with vesicular pleomorphic nuclei, and abundant eosinophilic cytoplasm and keratinization were noted(Figure 2 A & B). A typical mitosis and foci of necrosis noted.
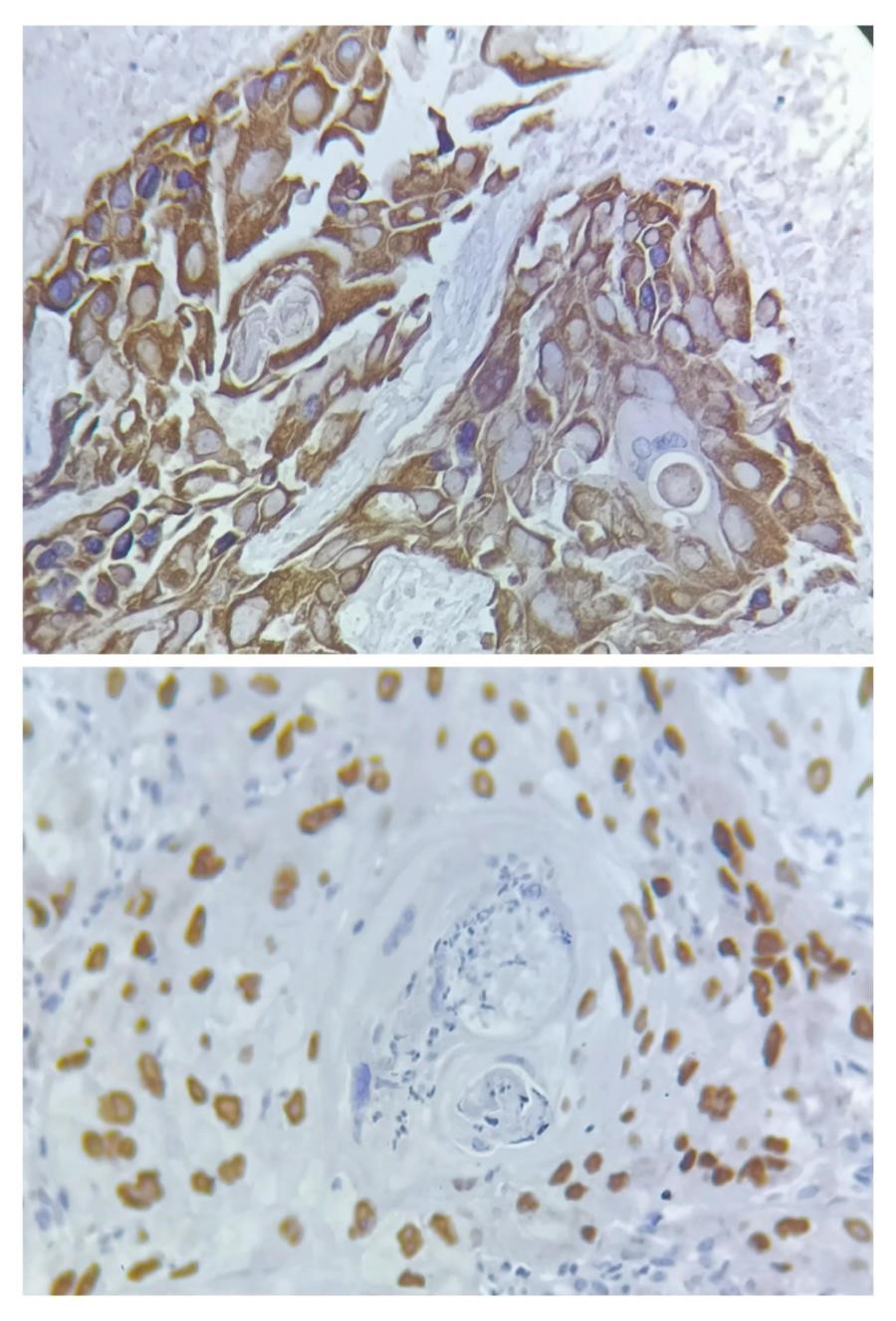
On immunohistochemistry, the tumor cells were diffusely positive for p40 and CK5/6.(Figure 3).


Discussion
Primary squamous cell carcinoma of the duodenum is extremely rare; only a few rare case reports have been published. Adenocarcinoma and neuroendocrine tumors are more common in the duodenum.
There is no definite explanation available for this, but certain theories have been proposed, such as tumors arising from nests of ectopic squamous cells, proliferation of undifferentiated basal cells of the duodenum into squamous cells, and squamous metaplasia secondary to chronic mucosal damage.
Also, squamous differentiation seen in adenocarcinoma and multipotent stem cells seen in the gastrointestinal tract can give rise to squamous cell carcinoma. 9
The present case, the tumor shows keratinization and intercellular bridges, which is fulfilling the criteria for squamous cell carcinoma. There was no other differentiation like adenocarcinoma component.
The imaging(PET SCAN) also showed circumferential solid tumors located in the second part of the duodenum without any other lesions in the rest of the body, including the lungs, urinary bladder, esophagus, and head and neck, which are the potential sites of SCC. The patient was evaluated clinically in the head and neck region for any other lesions. The oral cavity, buccal mucosa, tongue, gingivo-buccal sulcus, retromolar trigone, and palatal mucosa surfaces were all normal in appearance. No lymphadenopathy was identified in the neck. By considering imaging findings and clinical examination findings, metastasis was ruled out, and primary duodenal squamous cell carcinoma was considered.
The present case, the tumor shows keratinization and intercellular bridges, which is fulfilling the criteria for squamous cell carcinoma. There was no other differentiation like adenocarcinoma component.
There was an interesting tumor reported back then by Barnhill et al. in which the tumor showed trilinear differentiation that is adenocarcinoma component, squamous cell carcinoma component, and neuroendocrine component. They proposed that the tumor was the result of pluripotent stem cells located in the duodenum, which are capable of differentiating into different cells types. 10, 11
Although the pathogenesis of squamous cell carcinoma in duodenal mucosa(Figure 1A & B) was difficult to explain They might arise from congenital malformations such as diverticula and duplications of intestinal mucosa. 12
Shin T Zaw et al. Described metastatic squamous cell carcinoma in duodenum with primary site in esophagus. Primarily duodenal mass was identified and on through examination esophagus revealed an ulcerated lesion. Both the lesions showed poorly differentiated SCC. This case indicated the possibility of metastasis. 13
Baoshan Wang et al. described a case of SCC in periampullary region in advanced stage which was showing upregulation of PD-LI expression. The patient was given combined therapy with chemotherapy and immunotherapy(pembrolizumab) and the patient responded well. 14
Documentation of this rare tumor will give a rare possibilities of tumor morphology and better understanding of underlying pathogenesis and accordingly the treatment will be planned for better management of patient.
Conclusion
The incidence of SCC in gastrointestinal tract is very low. So the clinician must be aware of the possibilities of primary as well as metastasis. For which the patients must be evaluated for any hidden primary. A comprehensive correlation of clinical, radiological, Histopathological and Immunohistochemistry is required for accurate diagnosis and better treatment of patients.