- Visibility 123 Views
- Downloads 24 Downloads
- Permissions
- DOI 10.18231/j.jdpo.2024.036
-
CrossMark

Giant cell rich variant of extraskeletal osteosarcoma: A rare case report
- Author Details:
-
 Sebina Asmi A T *
Sebina Asmi A T *
-
P S Jayalakshmy
-
Aysha Shaheeda
Abstract
Extraskeletal osteosarcoma (ESOS) is an aggressive malignant tumour, producing neoplastic osteoid without attachment to the bone or periosteum. It can occur anywhere in the body including soft tissue, mesentery and retroperitoneum. It accounts for less than 1% of all soft tissue sarcomas. Subcutaneous ESOS and Giant cell rich subtype has an extremely rare incidence. Here we present the case of a 40 years old woman who presented with giant cell rich variant of extraskeletal osteosarcoma located in the subcutaneous plane of left thigh.
Introduction
Unlike osteosarcoma of bone in the younger age group, extraskeletal osteosarcoma (ESOS) are encountered in patients after 40 years. Subcutaneous ESOS may develop at a younger age compared to deep seated ESOS. Although majority of ESOS are reported in the extremities, subcutaneous ESOS can occur in other sites like trunk, scalp and abdominal wall. The etiology of ESOS is not completely known, proposed theories of development includes preceding trauma and radiation exposure. The overall survival of ESOS is poor, however survival rates of subcutaneous ESOS are comparably better than deep seated ESOS. The primary treatment involves surgical resection with wide resection margins and adjuvant chemoradiation.
Case Presentation
40 years old female presented with swelling over lateral aspect of left thigh for 6 months. Swelling was gradually increasing in size and was associated with pain. On examination swelling was 6x4 cm in size, non-tender with restricted mobility. MRI showed subcutaneous well defined focal lesion along posterolateral aspect of left mid-thigh suggestive of malignant lesion ([Figure 1]). Fine needle aspiration cytology was done and smear findings are that of Soft tissue sarcoma with multinucleated giant cells. Wide local excision was done and specimen sent for histopathological examination.
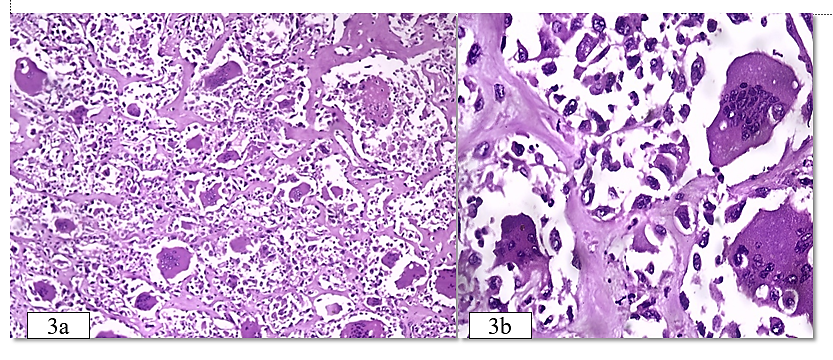
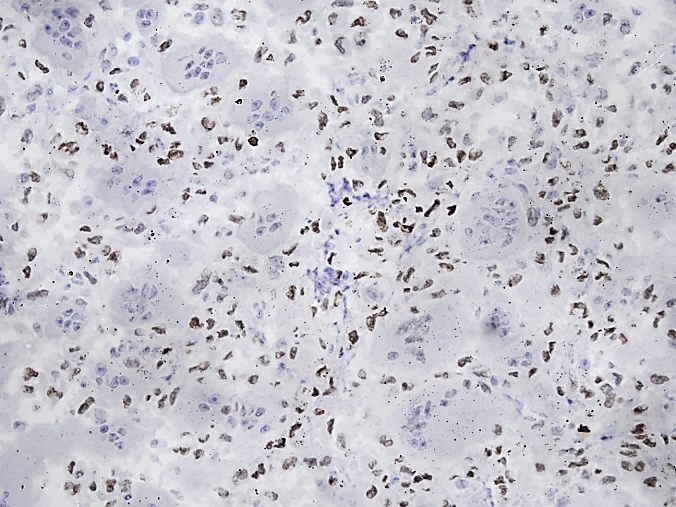
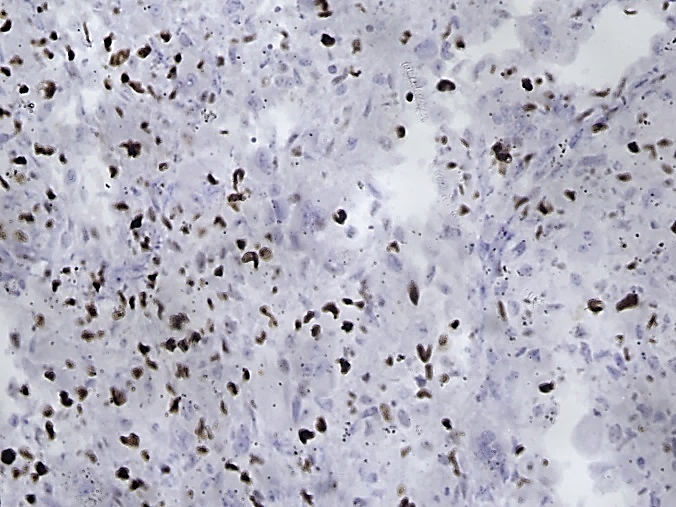
Grossly received skin covered excision specimen, cut section of which showed a circumscribed grey white firm lesion with areas of haemorrhage and necrosis measuring 6x5x4.5cm ([Figure 2]). Microscopic examination showed an infiltrative neoplasm composed of oval to spindle cells arranged in diffuse sheets with numerous multinucleated giant cells in between. Individual tumour cells have moderate cytoplasm, pleomorphic hyperchromatic nucleus with bizarre forms. Osteoid formation and neoplastic bone formation by tumor cells seen ([Figure 3]). Mitosis 8-9 per mm2. Areas of necrosis (<50%) and hemorrhage seen. Immunomarkers for SATB2 ([Figure 4]) and CDK4 were positive in tumour cells. MDM2 was negative. Proliferation index with Ki67 ([Figure 5]) was high (40%), hence the case was diagnosed as giant cell rich variant of ESOS.


Discussion
Extraskeletal osteosarcoma (ESOS) is a rare soft tissue tumor, most often located in the deep soft tissues of the extremities. Common locations of ESOS are deep soft tissue of the thigh, upper extremity and retroperitoneum. ESOS occurring in the subcutaneous tissue is extremely rare, seen in <10% of the cases. Computed tomography (CT) and magnetic resonance imaging (MRI) are preferred radiological investigations in case of ESOS. CT may show central calcification within the lesion, but its absence does not exclude the diagnosis. In MRI lesion is hypointense on T1 weighted images and hyperintense on T2-weighted images.The primary treatment involves surgical resection with wide resection margins and adjuvant chemoradiation. [1]
The histological variants of ESOS consist of osteoblastic variant, chondroblastic variant, fibroblastic variant, giant cell rich variant, telangiectatic variant, and small‑cell varaint, among which osteoblastic being the most common subtype. Giant cell-rich osteosarcoma, is a rare variant of osteosarcoma. Giant cell rich osteosarcoma contains a large number of benign and malignant multinucleated osteoclastic giant cells. Giant cell rich osteosarcoma can easily be mistaken for giant cell tumour due to the histological similarity. [2] Special AT-rich sequence-binding protein 2 (SATB2) is a sensitive marker for osteoblastic lineage and is positive in malignant bone and soft-tissue tumors with osteoblastic differentiation or bone formation. In a study conducted by Conner and Hornick 89% cases of ESOS were positive for SATB2. [3]
Metastatic osteosarcoma has to be ruled out before making the diagnosis of primary ESOS. In our case, clinical examination and other investigations did not identify any other mass or lesion in bone and other organs. Primary ESOS has also be differentiated from radiotherapy-induced osteosarcoma. Development of osteosarcoma after radiation depends on factors like dosage of radiation, associated chemotherapy, age of the patient, and genetic susceptibility to oncogenesis. Majority of radiation induced osteosarcoma arise from bone, but radiation-induced extraskeletal osteosarcoma has also be reported. Our patient had no history of radiotherapy, thus excluded radiotherapy-induced ESOS. [4], [5]
ESOSs are generally present as large tumour masses with an average diameter of 9 cm. Tumour size is the most important prognostic factor, as the patients with lesions >5 cm have a bad prognosis. [6] Giant cell rich ESOS has a poor prognosis, the overall 5 years survival rate is 25% to 66%. [7] Local recurrence and metastasis are common, the lung is the most common site of metastasis and so the close follow up of the patient is necessary. [8] Usually local recurrences and distant metastases are reported within 3 years. Role of other clinico-pathologic prognostic factors like histologic subtype, mitotic rates, cellularity, nuclear pleomorphism, tumour necrosis, initial treatment, and presence of metastases at diagnosis are under debate. [9], [10] The survival rates of subcutaneous ESOS are comparably better than deep seated tumours, may be due to earlier diagnosis and prompt treatment in case of the superficial lesion. [11]
Conclusion
The giant cell rich variant of ESOS is a rare malignant mesenchymal tumour of the soft tissue. Clinico-radiological correlation, histopathological analysis and immunohistochemical testing help to confirm the diagnosis of this tumour. Due to high risk of recurrence and metastasis, early detection is critical for effective management. Surgery and chemotherapy are the standard treatment options and close monitoring of patients after treatment is necessary.
Conflict of Interest
None.
Source of Funding
None.
References
- Tamura T, Suzuki K, Yasuda T, Nogami S, Watanabe K, Kanamori M. Extraskeletal osteosarcoma arising in the subcutaneous tissue of the lower leg: A case report and literature review. Mol Clin Oncol. 2018;9(3):287-92. [Google Scholar]
- Chobpenthai T, Thanindratarn P. Giant Cell-Rich Variant of Extraskeletal Osteosarcoma Above the Patella – A Rare Case Study and Review of the Literature. Biomed J Sci Tech Res. 2019;19(5). [Google Scholar] [Crossref]
- Sneha K, Joseph L, Susruthan M, Ramya R. Subcutaneous extraskeletal osteosarcoma of the foot: A case report. Sri Ramachandra J Health Sci. 2021;1(1):25-7. [Google Scholar]
- Saadaat R, Abdul-Ghafar J, Din N, Haidary A. Anal extraskeletal osteosarcoma in a man: a case report and review of the literature. J Med Case Rep. 2020;14(1). [Google Scholar] [Crossref]
- Papalas J, Wylie J, Vollmer R. Osteosarcoma after radiotherapy for prostate cancer. Ann Diagn Pathol. 2011;15(3):194-7. [Google Scholar]
- Hoch M, Ali S, Agrawal S, Wang C, Khurana J. Extraskeletal osteosarcoma: A case report and review of the literature. J Radiol Case Rep. 2013;7(7):15-23. [Google Scholar]
- Torigoe T, Yazawa Y, Takagi T, Terakado A, Kurosawa H. Extraskeletal osteosarcoma in Japan: Multiinstitutional study of 20 patients from the Japanese musculoskeletal oncology group. J Orthop Sci. 2007;12(5):424-9. [Google Scholar]
- Aden D, Zaheer S, Ranga S. Giant cell variant of extraskeletal osteosarcoma. Arch Med Health Sci. 2023;11(2):281-3. [Google Scholar]
- Hussain M, Al-Akeely M, Alam M, Jasser N. Extraskeletal osteosarcoma, telangiectatic variant arising from the small bowel mesen tery. Saudi Med J. 2011;32(9):958-61. [Google Scholar]
- Oh S, Chang H. Unusual giant cell-rich variant of extraskeletal osteosarcoma in the mesentery of small intestine. Int J Clin Exp Pathol. 2017;10(11):11225-9. [Google Scholar]
- Healy C, Kahn L, Kenan S. Subcutaneous extraskeletal osteosarcoma of the forearm: A case report and review of the literature. Skeletal Radiol. 2016;45(9):1307-11. [Google Scholar]