Introduction
Uterine carcinosarcomas are rare tumors that make up fewer than 5% of all uterine malignancies. These tumours, which were formerly known as malignant mixed Müllerian tumours, are dedifferentiated carcinomas that originate from a single malignant clone and contain both carcinomatous (epithelial) and sarcomatous (Mesenchymal) features.1
Compared to other endometrial cancers, it is more frequently identified at an advanced stage. The epithelial component is the most dominant and is typically a high-grade histotype (which can be serous, endometrioid, clear cell, mixed, or undifferentiated), In contrast, the sarcomatous component may be homologous (leiomyosarcoma, fibrosarcoma, endometrial stromal Sarcoma) or heterologous (Rhabdomyosarcoma, chondrosarcoma, Osteosarcoma), based on how much the mesenchymal component mimics the uterine tissues. About 40% of endometrial carcinosarcomas exhibit heterologous differentiation, which is linked to a worse prognosis when compared to homologous changes.2 We present here a case of 77 year old female with carcinosarcoma showing serous carcinoma as epithelial component with homologous and heterologous components like endometrial stromal sarcoma and chondrosarcoma as sarcomatous components along with heterologous bone formation who had poor outcome on follow up.
Case Presentation
A 77-year-old female patient presented to our hospital with complaints of mild lower abdominal pain, which was of dragging type. Patient is a known case of hypertension and was on regular medication.
Endometrial curettage was performed and the tissue sample was sent for histopathological examination which showed a malignant neoplasm composed of round to polygonal cells arranged in sheets, clusters, and singles and around the blood vessels. Most of the tumour cells show scant eosinophilic cytoplasm with few tumour cells showing abundant clear vacuolated cytoplasm. Nuclei were vesicular to hyperchromatic with moderate pleomorphism with numerous atypical mitoses. Also seen are areas showing edema, fibrinoid necrosis, and haemorrhage. No epithelial component was identified in the curettage specimen and was reported as poorly differentiated malignancy. On IHC the tumor cells showed focal positivity for cytokeratin, cyclin D1 and CD10 and was reported as undifferentiated carcinoma. The patient further underwent Extra-fascial Hysterectomy with Bilateral salpingo-oophorectomy.
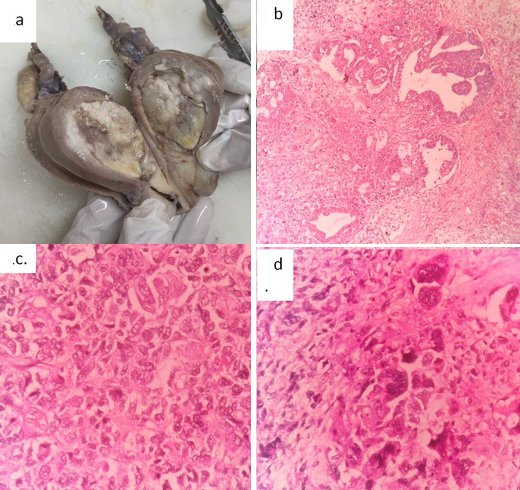
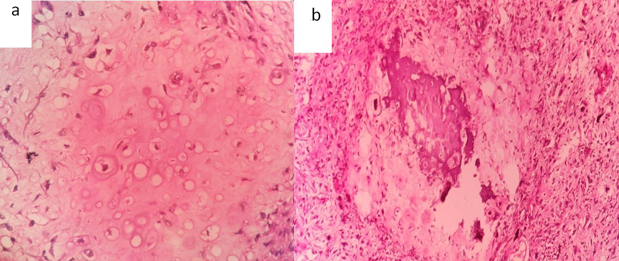
On examination Cervix appeared unremarkable. Endometrium appeared dilated and showed a grey white to tan, friable, polypoidal mass measuring 4.5x4x3cm filling the entire endometrial cavity (Figure 1a). On microscopy it showed malignant epithelial component with papillary, glandular and cribriform pattern (Figure1b) and tumor cells composed predominantly of sheets of dyscohesive cells (Figure 1c), focally exhibiting severe pleomorphism with bizarre nuclei (Figure 1d), areas of myxoid change with chondrosarcomatous differentiation (Figure 2a) and heterologus bone formation (Figure 2b). The individual tumor cells showed vesicular nucleus with prominent nucleoli, increased mitosis with large areas of necrosis. The adjacent endometrium showed focus of serous intraepithelial carcinoma and atrophy. Myometrial invasion was present involving more than half of the myometrium with lymphovascular invasion. Hence a final diagnosis of carcinosarcoma was made with serous carcinoma as epithelial component and undifferentiated sarcoma, chondrosarcoma as sarcomatous elements. The patient presented with malignant pleural effusion with a period of one month on follow up and finally succumbed to the disease.
Figure 1
a: Gross image showing dilated endometrial cavity with a friable, polypoidal mass; b: Histopathological examination showing epithelial component arranged in glandular pattern (H&E, 100X); c and d: Undifferentiated sarcomatous component arranged in sheets (c) and bizarre forms (d) (H&E, 400X)
Discussion
Carcinosarcoma of the uterus, previously known as malignant mixed Müllerian tumor (MMMT) is a uncommon, typically aggressive neoplasm that accounts for less than 5% of all uterine carcinomas with exceedingly dismal prognosis. 3 Because this tumour has an epithelial component, it differs from other uterine sarcomas fundamentally, and this carcinomatous component is what distinguishes carcinosarcoma from other uterine sarcomas. 4
When a patient presents with signs of endometrial cancer, the local extent of the illness is often assessed using either gadolinium-enhanced magnetic resonance imaging (MRI) or computed tomography (CT) scanning. Carcinosarcoma appears on CT or MRI as a heterogeneous bulky polypoid mass with prolonged intense enhancement that typically prolapses into the endocervical canal. Additionally, both modalities are capable of identifying nodal involvement, myometrial invasion, and the existence of metastatic disease.1
The mesenchymal components of homologous uterine carcinosarcomas are made of tissues typically seen in the uterus called intrinsic differentiation. Endometrial stromal sarcoma, undifferentiated sarcoma, fibrosarcoma, leiomyosarcoma, or a combination of these entities may also be the homologous mesenchymal component. The heterologous type may contain sarcomatous elements, which are often absent from the uterus in their benign state called extrinsic differentiation. They include chondrosarcoma and rhabdomyosarcoma, which occur more frequently, and liposarcoma and osteosarcoma, which occur less frequently.
The carcinomatous (malignant epithelial) component typically has glandular origins. But there are also non-glandular components like squamous cell or undifferentiated cancer. In most cases, the glandular component correlates with endometrioid endometrial cancer; in a smaller number of cases, it may also have serous or clear cell morphology. Ali Kord et al.5 reported a case of uterine carcinosarcoma with infiltrating malignant high-grade carcinoma of endometrioid differentiation and undifferentiated sarcomatous component. Desai GS et al.6 reported a case of uterine carcinosarcoma with endometrioid type carcinomatous element . Adachi et al.7 reported serous carcinoma and homologous sarcomatous elements. Lai-tiong reported chondrosarcomatous elements in uterine carcinosarcoma.8 Serous carcinoma being the epithelial component with heterologous chondrosarcomatous component are rare associations as seen in our case.
It might be challenging to distinguish between uterine sarcoma and carcinosarcoma with a prominent mesenchymal component (sarcomatous overgrowth), which emphasises the significance of a thorough pathological-anatomical work-up. Before undergoing definitive surgery, endometrial sampling either endometrial biopsy or dilatation and curettage is often carried out. But that sampling might not be a reliable technique for uterine carcinosarcoma diagnosis. Therefore, further work-up is necessary if endometrial sample is negative but clinical suspicion is still high. The definitive diagnosis of carcinosarcoma usually depends on pathologic examination after hysterectomy, since the diagnosis is based on histologic evidence of a dual population of carcinomatous and sarcomatous cells with infiltration of the stroma.1 This case also had the same difficulty with predominance of mesenchymal elements with no carcinomatous elements represented in curetting leading to diagnosis of Undifferentiated carcinoma even after IHC. Which on hysterectomy showed differentiated serous elements and Chondrosarcomatous elements and was finally diagnosed as carcinosarcoma.
Compared to other endometrial cancers, it is more frequently identified at an advanced stage. 2 Considering the highly invasive nature of uterine carcinosarcomas, early detection and correct diagnosis via characteristic imaging and pathology findings, as well as choosing the correct treatment approach are of extreme importance to improve the patient’s survival. 5, 9
Conclusion
This is a case report of uterine carcinosarcoma with rare epithelial and sarcomatous components with heterologous bone formation. This case highlights the importance of extensive sampling in case of polypoidal tumors to prevent misdiagnosis especially when the tumor is mesenchymal predominant which can help to start early treatment. Also, this case report reiterates the poor prognosis associated with the disease.