Introduction
Mycetoma is a chronic suppurative disease mainly affecting the skin and subcutaneous tissue and is characterized by a triad of swelling, draining sinus and grains.1 Mycetomas are caused by different species of fungi and bacteria including actinomycotic mycetoma which is caused by aerobic species of actinomycetes while eumycotic mycetoma is caused by a variety of fungi, most common being Madurella mycetomatis.2 There is an inter-country and regional variation in the species responsible for mycetoma, with Nocardia species and Madurella grisea being the most common causes of mycetoma in the Indian subcontinent.3 Overall, most arid and hot climates having short seasons of heavy rainfall harbour maximum cases, with Actinomycetoma being more prevalent in drier areas and eumycetoma being more common in areas with rainfall.3 In most cases of Mycetoma lower extremity is involved with foot (70%) being most commonly involved followed by hand. Other sites like the head, neck, chest, shoulder, and arms have also been reported.4 The incubation period for the disease is variable ranging from 3 months to 9 years.4 A combination of diagnostic investigation is essential to identify the causative organism and extent of the disease.5 The Final treatment regimen depends on the causative organism and the stage of disease, in the case of Actinomycetoma antimicrobial combination therapy is used while eumycetoma usually required a combination of antifungal medications and surgical intervention.6 If Untreated mycetomas undergo a slow destructive progression leading to deformities and amputation. 7
Materials and Methods
This study was a three-year retrospective and two-year prospective study conducted on 34 patients in the Department of Pathology and Microbiology to study the clinicopathological spectrum of mycetoma and its diagnostic features. A detailed clinical history including age, gender, site involved, family history, and occupational exposure was taken. Further examination was done for any associated lymphadenopathy. All the relevant radiological investigations including the X-rays, CT scan and MRI were recorded wherever available. Fine Needle Aspiration was done with a 22 gauge needle under negative pressure from the suspected mycetoma lesion under aseptic condition. Material aspirated was both air-dried and fixed and MGG (May Grunwald and Giemsa) and PAP staining were examined under a microscope to make a presumptive diagnosis. This was followed by the procedure of deep biopsy/excision biopsy (in cases with negative FNAC findings and positive cytology findings, to confirm the results. The obtained tissue was further processed for a histopathological examination and grains, if obtained were grossly examined followed by a direct microscopic examination and culture. Biopsy obtained was fixed in a 10% formula line followed by dehydration by different concentrations of ethanol, clearing by Xylene, impregnation and embedding by using paraffin wax (a 2- to 5-micron-thick section obtained by microtome), and finally staining with Hematoxylin and Eosin Stain. Primary identification of the causative agent was done on H and E-stained smears. Further special histochemical stains like Zeihl Neelson (ZN) Stain, Gram stain and PAS stain were done for further characterisation (Actinomycetoma being gram-positive and ZN positive, while eumycetoma being PAS positive). Culture of Grain was done by using Modified Sabouraud agar supplemented with 0.5% yeast extract and Lowenstein agar to identify the specie. Statistical Analyses including sensitivity, specificity and diagnostic accuracy of detection by cytology and histopathology were calculated by SPSS 2.0 software. Ethical clearance was taken from the Institutional Ethical Committee.
Observations and Results
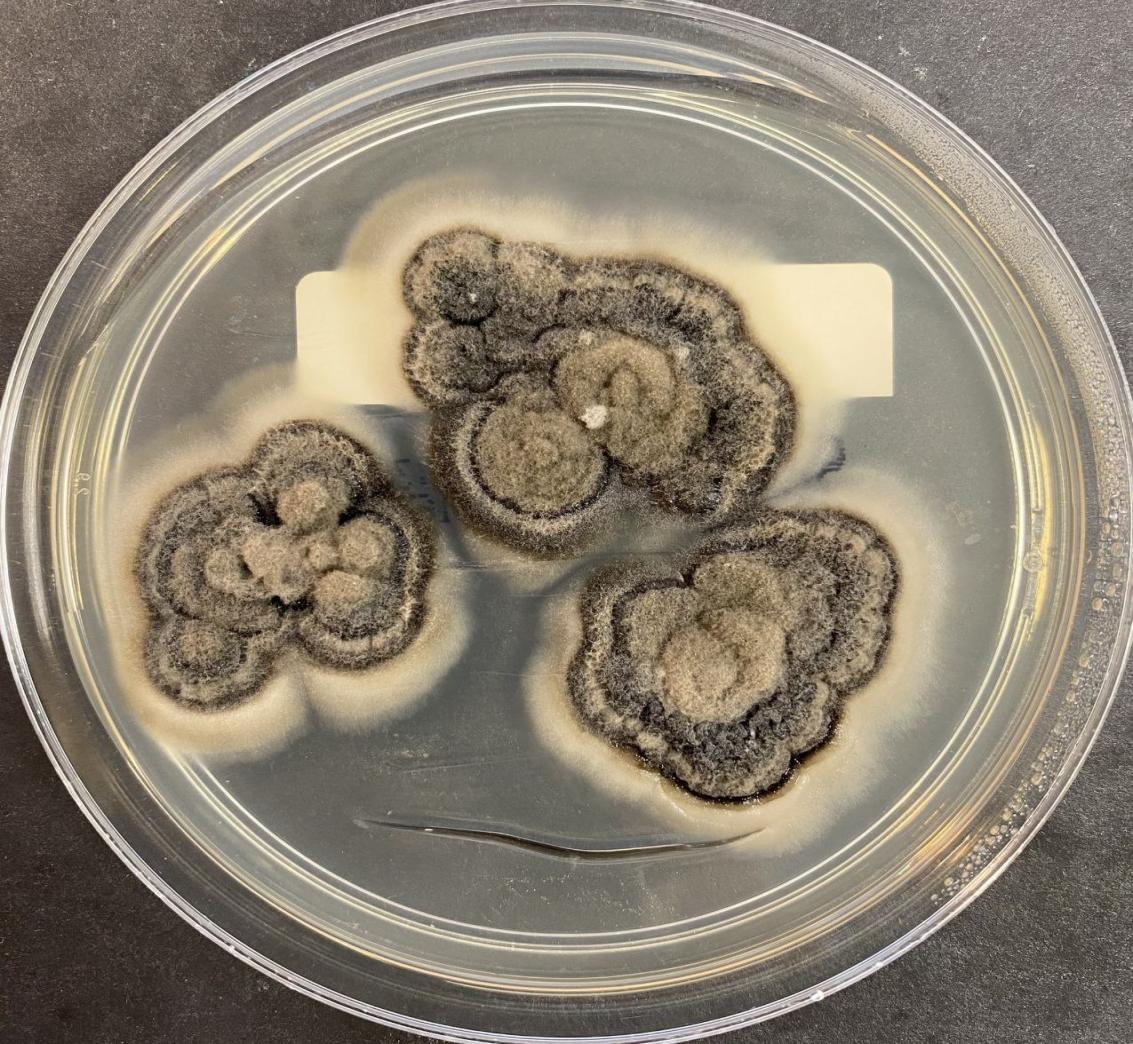
This study was a three-year retrospective and two-year prospective study including a total of 34 cases of mycetoma over 3 years. There were 25(73.5%) males and 9 (26.5%) females with a Male: Female Ratio of 2.7:1. Most of the patients were adults (20, 58.8%) belonging to the age group (19-60 years). This was followed by adolescents (14-18 years) and the elderly (>60 years) constituting 8(23.5%) and 4(11.9%) respectively. Least (2 cases, 5.8%) belonged to the Paediatric population (<13 years).Most common site affected was foot (14, 41.1%) followed by hand (10, 29.4%) and leg (6, 17.6%). 1 case (3%) was reported in Perineum and Chest. One patient had bilateral foot involvement. Most of the patients belonged to rural areas (85.2%) while the remaining (5, 14.8%) lived in urban areas. Most of the cases (17,50.2%) had a duration of >6 months and <1 year, followed by 9 cases (26.4%) which had a duration of 1 year to 5 years. 6 cases (17.6%) had a duration of fewer than 6 months while 2 cases (5.8%) had a duration of >5 years. When investigated it was found that about 10 cases (29.4%) had a positive family history with similar infections occurring within their families while the rest (24,70.6%) had a negative family history. Maximum patients (12,35.2%) did agricultural work for livelyhood.10 cases (29.4%) were labourers,8 (23.5%) were herdsmen, and 1 (3.1%) was a fisherman while 3 cases (8.8%) were not related to any occupational exposure. 29(85.2%) had a history of trauma while 5 cases (14.8%) has a negative trauma history. The most common presenting complaint was a painless mass seen in 28 cases (82.3%), followed by a discharging sinus (20, 58.8%) (Figure 1). Painful swelling was a complaint in 6 cases (17.6%).15 cases (44.2) demonstrated the presence of granules. 2 cases each (5.8%) presented with a plaque and abscess respectively, and 4 cases (9.2%) showed underlying bony destruction. Regional Lymphadenopathy was noted in 2 F cases (5.8%) while absent in the rest (32,94.2%). 20 cases (58.8%) had a history of chronic disease including Diabetes Mellitus (14, 41.1%), Tuberculosis (3, 8.8%),Chemotherapy (1,3%), HIV (1,3%), Covid 19 (1,3%) and 6 cases(17.6%) had a history of chronic smoking (>10 years), while 8 cases (23.5%) had no significant history. When Further studies were done to differentiate the causative organism 28 cases (82.3%) were of eumycetoma while 6 cases (17.6%) were of Actinomycetoma. 26 cases (76.4%) showed granules with colours ranging from black to brown to yellowish-white while 8 cases (23.6%) showed granules of pinkish-red colour. 26 cases (76.4%) showed granules with colours ranging from black-brown to yellowish-white (Figure 2) while 8 cases (23.6%) showed granules of pinkish-red colour (Figure 3 ) Plain radiographs showed different translucent areas and sclerosis of involved sites with occasional snow melting appearance in some. CT Scan showed the presence of air with a crescent shape between the mycetoma and the wall of the cavity showing a crescent sign. MRI features collectively revealed rounding of soft tissue mass in the subcutaneous plane with multiple, small, round and discrete hypointense lesions measuring averagely around 1-8 separated by a low-signal-intensity rim, while some lesions show hyperintensity with a central low-signal-intensity dot (Figure 4). Fine needle aspiration was able in correct specie identification in 28 cases with a sensitivity of 82.35%, Specificity of 94.4% and diagnostic accuracy of 88.5%. Most of the smear shows singly scattered as well as clusters of mixed inflammatory infiltrate comprising neutrophils, lymphocytes with fibrillary clusters of the organism or branching fungal hyphae while necrotic granular debris was also noted in a few cases (Figure 5). Histopathology was able to identify 32 species correctly with a specificity of 94.1 %, specificity of 97.1% and diagnostic accuracy of 95.6%.H and E stain section on microscopy showed suppurative granulomas composed of neutrophils, lymphocytes, plasma cells and occasional giant cells with characteristic grains of the species in the centre. The grains of Eumycetoma was, brown and large with a filamentous type of brown septate and hyphae arranged radially at the periphery and haphazardly in the centre. Histological sections from actinomycotic mycetomas showed both large and small-sized round and multilobed grains with a paler centre and dark basophilic periphery. (Figure 6). When further studies (culture of grains, Special stains including PAS and ZN Stain) were done to differentiate the causative organism 28 cases (82.3%) were of eumycetoma while 6 cases (17.6%) were of Actinomycetoma (Figure 7, Figure 8).

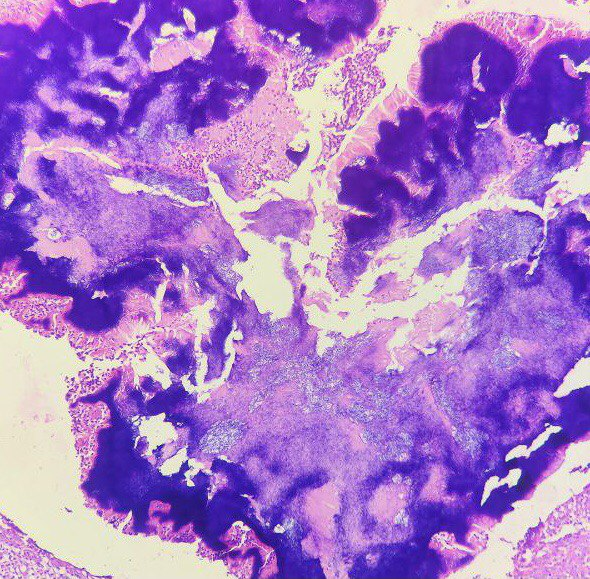
Figure 2
Brown granules of madurella mycetoma in the centre surrounded by giant cells and chronic inflammatory infiltrates (Hematoxylin and Eosin stain, X10).
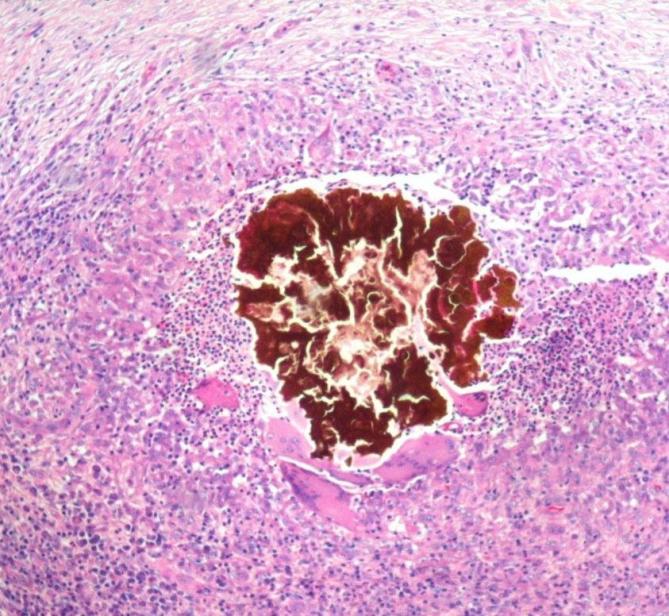
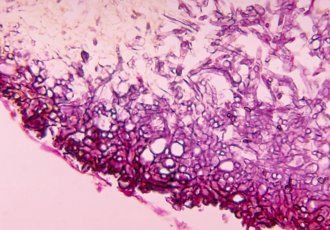
Figure 3
Pinkish brown granules of Actinomadura madurae in the centre surrounded by inflammatory cells (Hematoxylin and Eosin stain, X10).
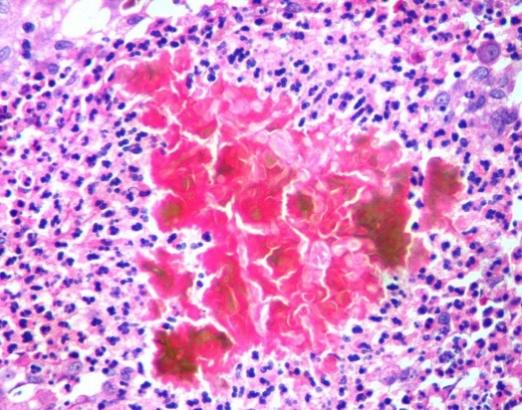
Figure 4
MRI of the foot showing characteristic dot in circle sign (arrow). The high-intensity circles correspond to granuloma and the central low-signal dots correspond to bacterial or fungal grains.
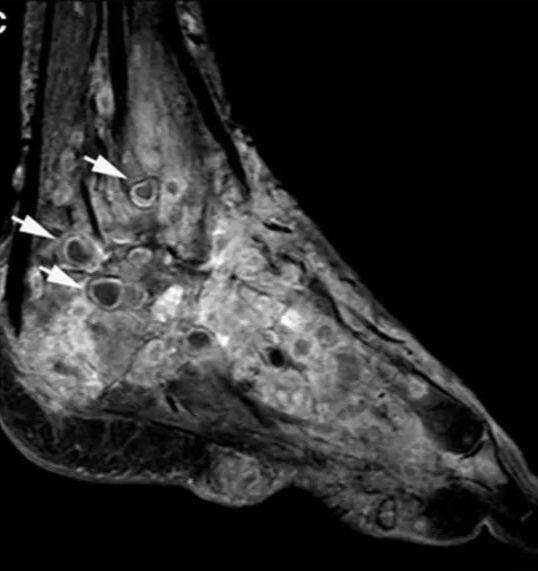
Figure 5
Fine needle aspiration cytology smear showing clumps of filamentous projections of Actinomyces (arrow) (May Grunwald Giemsa Stain, X10).
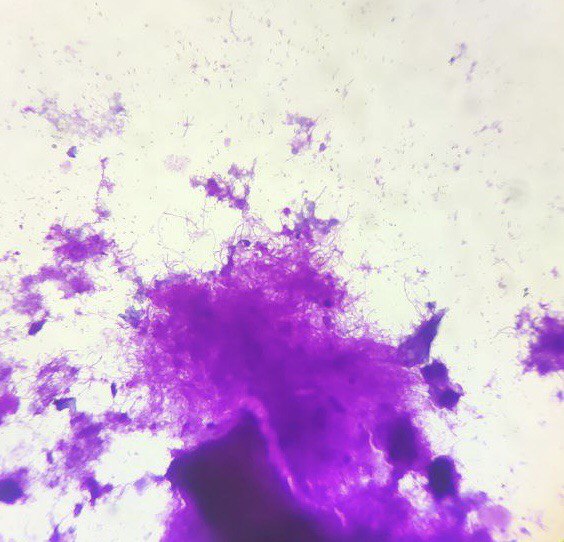
Figure 6
Histological sections showing multilobulated colonies of actinomycetoma with peripheral basophilia (short arrow) knobby projections and surrounded by inflammatory.
Discussion
This study was conducted in the northeast part of India which lies in the not-so-common belt for mycetoma, which will help in the addition of literature. In India, Rajasthan (North-West India) and South India are most affected.8 In the total span of the study, a total of 34 cases were studied. Males had a greater dominance of disease as compared to females. This could be due to the higher number of males having occupational exposure as well as the inhibitory effect of progesterone over the growth of the organism 1 though further studies are required to verify the same. Mycetomas can affect all age groups, but Adults are commonly affected usually between the age group of 20 and 40 years.9 Any site may be affected in mycetoma but the lower limbs are found to be the most affected part in the majority of cases.1 Mycetomas are considered occupational diseases of individuals who work in rural areas, such as farmers and shepherds or that engage in activities related to the environment.10 The incubation period is usually variable from 3 months to 9 years and due to such a long incubation period, the actual history of causative risk factor is difficult to establish.4 Most of the cases in our study were from the rural areas this could be due to their surrounding unhygienic living environment comprising of homes constructed with mud, dried animal dung, thorns and trash, moreover walking barefooted and fungus in excreta or dung may also be possible contributing factors.11 The role of genetic susceptibility in the development of mycetoma is still under study, in our study, 29.4% of the patients had a positive family history which could be possibly due to exposure to the same epidemiological risk factors or sharing genetic and familial factors.11 The classic clinical presentation of mycetoma includes a triad of painless subcutaneous swelling with multiple sinus formations and a purulent discharge containing characteristic grains in most cases.12 These granules show a characteristic size, colour and consistency which gives a clue about the etiological species. As the disease progresses the formed papules and pustules undergo a breakdown to form draining sinuses.12 5.8% of the cases showed the involvement region involved. This could be explained by the spread of the infection which usually occurs mostly through the lymphatics, although haematological spread can also occur.13 In concomitant comorbid and associated conditions including Diabetes mellitus, malnourishment, malaria, HIV/AIDS, leishmaniasis, diabetes mellitus a faster progression of the disease is noted which may be due to weakening of innate immunity defence in such condition.14 A combination of various diagnostic methods helps to establish the diagnosis of mycetoma which includes microscopic examination of grains, fine needle aspiration cytology, histopathology and culture with the addition of newer diagnostic tests like serology and molecular tests if needed.15 Specimen collection included the collection of discharging fluid or aspiration, scrapings of sinus walls and tissue biopsy while spontaneously extruded grains usually contain dead organisms and should not be considered for evaluation should be examined for the presence of grains.15 These grains can be evaluated by clinically observing the size, colour and consistency of the particular agent which helps in a rapid but provisional diagnosis which should be followed by grams staining and microscopic evaluation which plays a vital role in distinguishing between actinomycetoma and eumycetoma. In cases where no draining sinus is seen, aspiration cytology followed by deep biopsy helps in establishing the diagnosis. Histopathological findings include granulomas with mixed inflammatory infiltrates and characteristic grains usually showing branching and septations, special stains like PAS and ZN further help in the differentiation of species.16 Grains of many species have overlapping morphological features, in such cases culture in special media such as Lowenstein–Jensen media, Sabouraud agar 4%, help in the accurate diagnosis. identification of the causative agent.17 Newer diagnostic tests including immunoblots, indirect hemagglutination assays, immunodiffusion, counterimmunoelectrophoresis and ELISA can detect early stages of the disease even before granule formation but are not used presently and their use is limited to epidemiological studies.18 Disease extent and bony involvement can be detected by radiology, and ultrasonography further can differentiate between mycetoma, osteomyelitis or any tumour. Subtle differences between actinomycetoma and eumycetoma can also be picked up. Helical computerized tomography and MRI are most sensitive in detecting early changes along with picking up diagnostic signs like “dot-in-circle sign”.19, 20 Treatment strategies largely depend on the final diagnosis defining the underlying etiological agent whether fungi or bacteria as actinomycetoma is treated with antibiotics while eumycetoma is treated with a combination of antifungals and surgical excision, though prolonged is needed in both. 21
Conclusion
Early recognition of clinical features with timely diagnosis using a combination of techniques followed by initiation of appropriate therapy is of utmost importance to prevent the destruction, morbidities or amputation of vital human organs for a disease that is completely benign and curable. Moreover, social awareness and education of people at risk are equally important so that they can identify the risk factors, predisposing conditions and associated symptoms and seek timely help to prevent lifelong damage. Further, the development of more cost-effective, rapid and field-friendly diagnostic methods especially for high-prevalence areas would prove to be a boon for this neglected disease.
Limitations
However, the study has limitations inherent to its design and there may be limitations of generalisation of results to other geographic areas of the world. Different diagnostic methods have their limitations like direct microscopic examination of grains is a rapid method but lacks accuracy. FNAC technique is simple, quick, and economical but may be painful in some patients and may induce infection and cellulitis in some cases. Serodiagnostic tests were not employed in the present study as they are tedious and lengthy and may lead to false positive cross-reactivity between different mycetoma causative organisms. Newer Molecular methods like PCR help in the accurate diagnosis of species but they are quite expensive.