- Visibility 16 Views
- Downloads 4 Downloads
- DOI 10.18231/j.jdpo.2022.037
-
CrossMark

Respiratoryepithelialadenomatoid hamartoma (REAH)
Dear Sir,
Respiratory epithelial adenomatoid hamartomas (REAH) are rare, glandular proliferations of the respiratory tract lined by ciliated respiratory epithelium. It is often found incidentally and due to its low prevalence, are often misdiagnosed for other sinonasal masses. Clinically and radiologically it mimics inflammatory nasal polyps and true neoplasms like inverted papillomas and low-grade sinonasal adenocarcinomas. Histopathopathology is considered as gold standard in diagnosing this rare entity.
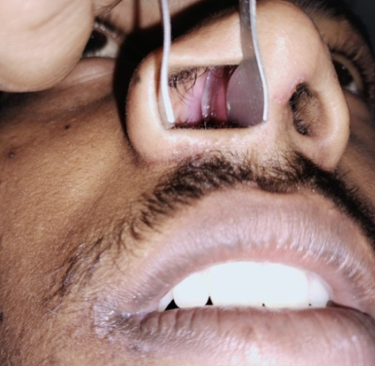
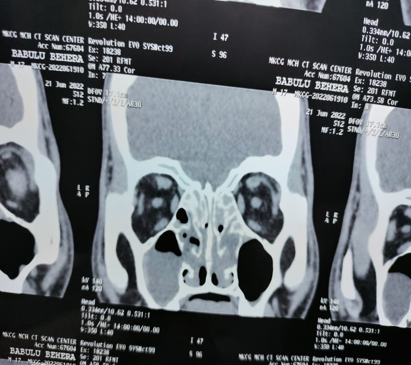
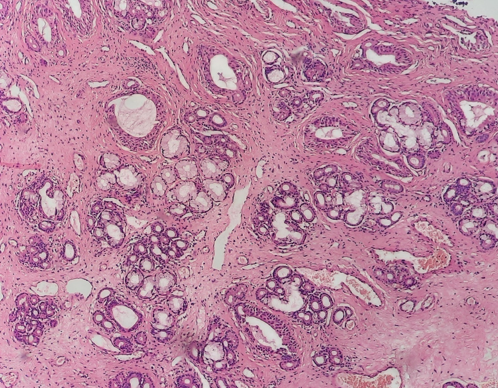
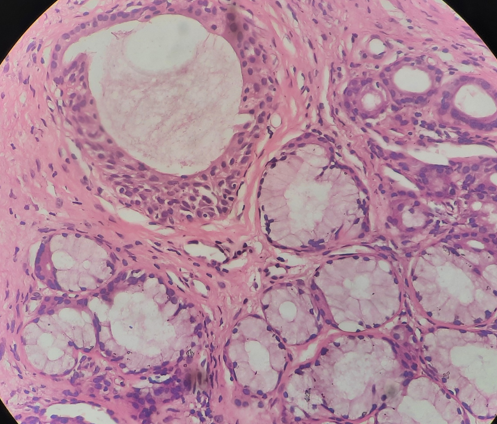
A 55yr old male presented to ENT OPD with complaints of bilateral nasal obstruction since a year associated with rhinorrhea on and off. There was no history of anosmia and no red flag symptoms in his history. On anterior rhinoscopy, he was found to have a bilateral, polypoidal mass arising from posterior nasal septum. The mass was pink in colour with a smooth surface and had skin changes. On probing the mass was nontender, was sensitive to touch, did not bleed and the root of the mass was not identified. The patient was posted for punch biopsy with an advice to do a CT scan. CT scan of the sinuses demonstrated a 5 cm large, lobulated soft-tissue mass lesion. Bilateral osteomeatal complex were blocked and there were features suggestive of pansinusitis. An Incisional biopsy of the lesion was performed and bits of tissue was send to our department for histopathological analysis with clinical diagnosis of Benign sinusoidal polyposis (? Fungal etiology). Grossly, we received bits of tissue with glistening surface altogether measuring 2x1x0.8 cm. Histopathology showed pseudostratified columnar respiratory lining epithelium with subepithelial tissue showing proliferation of seromucinous glands, blood vessels, fibrous tissue in a disorganosed manner. Few glandular epithelium showing ciliated pseudostratifiied columnar metaplasia. Thus a diagnosis of Respiratory Epithelial Adenomatoid Hamartoma was rendered on histopathology.[[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6]]


Respiratory epithelial adenomatoid hamartomas (REAHs) was first reported by Wenig and Heffner in 1995.[1] They are benign, glandular proliferations of the surface epithelium of the nasal cavity and paranasal sinuses. REAH occurs in adults mostly in 5th to 6th decade with a strong male predilection. [2] Many REAHs are found in the olfactory groove and associated with olfactory groove widening.[2], [3] Other common locations include the posterior nasal septum, lateral nasal wall, sinus cavities, and olfactory cleft. [4] Typical presenting symptoms include the following: nasal obstruction, nasal stuffiness, deviated septum, epistaxis, and chronic rhinosinusitis occurring from a few months to many years in duration.[5]
Although REAH have been reported in the past in numerous case reports however there is still an ongoing debate related to its etiology and pathogenesis. Two separate entities have been reported; one in association with nasal polyps, and other is solitary lesion, the latter being uncommon. However review of literature suggests that there is no clear etiologic factor in the development of REAH, but, the frequent association with nasal polyps suggests an inflammatory component.[6] Hawley et al. demonstrated a 79% polyp association in a series of 45 patients and similarily studies done by Lorentz et al demonstrated the presence of REAH in 48% of biopsied oedematous olfactory clefts associated with nasal polyps and thus been theorised that a state of chronic inflammation in the nasal cavity could have lead to the development of this lesion.[7], [8]
Differential diagnosis for REAH includes the following: inflammatory polyps, inverted papilloma, and low-grade adenocarcinoma.[9] The majority cases of REAH occurs in the nasal cavity mostly posterior nasal septum and is usually unilateral in comparison to nasal polyp that shows septal involvement and is bilateral. However in our case the mass was present bilaterally that lead the clinicians think, that it could possibly be a case of beingn sinonasal polyposis. Surface epithelium in REAH invaginates into submucosa and there is direct continuity with proliferating glands with no basement membrane thickening. Surface invagination in nasal polyp is absent along with absent glandular proliferation and basement membrane is characteristically thickened. Glands in REAH are widely spaced, small- to mediumsized, round to oval glands lined by respiratory epithelium admixed with goblet cells separated by edematous and fibrous stroma containing mixed inflammatory cells is the (dominant feature). Sometimes glands are usually distended with mucus. Other differential diagnosis is Inverted papilloma that arises from nasal cavity (maxillary sinus) and is rarely bilateral. Multiple inversions of the surface epithelium (hyperplastic squamous epithelium) with only few goblet cells, thin basement membrane, no to rare mucoserous glands are features of inverted papilloma. Adenocarcinoma on other hand is characterized by presence of back to back glands, occasional nuclear pleomorphism, prominent mitotic activity along with features of perineural invasion and desmoplastic stroma.
REAH is becoming a more widely recognized tumor. Treatment of REAH is usually curative with endoscopic resection and recurrence following is extremely rare. [7] REAHs are benign entities that should be included in the differential diagnosis for sinonasal masses. Expertise in Pathology is required for accurate diagnosis and to differentiate these lesions from nasal polyps and more aggressive pathologies, that would avoid unnecessary surgery.
Source of Funding
None.
Conflict of Interest
None.
References
- BM Wenig, DK Heffner. Respiratory epithelial adenomatoid hamartomas of the sinonasal tract and nasopharynx: a clinicopathologic study of 31 cases. Ann Otol Rhinol Laryngol 1995. [Google Scholar] [Crossref]
- W L Davison, A N Pearlman, L A Donatelli, L M Conley. Respiratory epithelial adenomatoid hamartomas: an increasingly common diagnosis in the setting of nasal polyps. Am J Rhinology Allergy 2016. [Google Scholar]
- JT Lee, R Garg, J Brunworth, DB Keschner, LDR Thompson. Sinonasal respiratory epithelial adenomatoid hamartomas: series of 51 cases and literature review. Am J Rhinol Allergy 2018. [Google Scholar] [Crossref]
- WG Albergotti, AJ Psaltis, RJ Schlosser. Respiratory epithelial adenomatoid hamartoma of the olfactory groove: A report of 4 cases and a review of the literature. Ear Nose Throat J 2016. [Google Scholar]
- BM Wenig, CDK Heffner, M Heffner. Respiratory epithelial adenomatoid hamartomas of the sinonasal tract and nasopharynx: a clinicopathologic study of 31 cases. Ann Otol Rhinol Laryngol 2016. [Google Scholar] [Crossref]
- G Gauchotte, B Marie, P Gallet, DT Nguyen, M Grandhaye, R Jankowski. Respiratory epithelial adenomatoid hamartoma: a poorly recognized entity with mast cell recruitment and frequently associated with nasal polyposis. Am J Surg Pathol 2013. [Google Scholar] [Crossref]
- KA Hawley, S Pabon, A P Hoschar, R Sindwani. The presentation and clinical significance of sinonasal respiratory epithelial adenomatoid hamartoma (REAH). Int Forum Allergy Rhinol 2013. [Google Scholar] [Crossref]
- C Lorentz, B Marie, J M Vignaud, R Jankowski. Respiratory epithelial adenomatoid hamartomas of the olfactory clefts. Eur Arch Otorhinolaryngol 2012. [Google Scholar] [Crossref]
- D Vira, S Bhuta, MB Wang. Respiratory epithelial adenomatoid hamartomas. Laryngoscope 2011. [Google Scholar]