- Visibility 46 Views
- Downloads 10 Downloads
- DOI 10.18231/j.jdpo.2021.033
-
CrossMark

Atrial myxoma- A case report with review of literature
Introduction
Atrial myxoma is the most common primary cardiac neoplasm. Over 72% of primary cardiac tumours are benign. In 7% it has genetic origin and arises as a component of heritable disorder with some clinical manifestations. The prevalence of cardiac tumours at autopsy is 0.001% to 0.3% in which more than 50% is myxoma.[1], [2]
These are the benign neoplasms arising from primitive multipotent mesenchymal cells. Two thirds of Carney Complex-associated cardiac myxomas exhibit mutations in PRKAR1A. PRKAR1A mutations occur in both familial and sporadic forms of CNC but have not been described in isolated (nonsyndromic) cardiac myxomas. Although sporadic myxomas do not show consistent genetic alterations, familial syndromes associated with myxomas have activating mutations in GNAS1 gene or null mutation in PRKAR1A. [3]
Case History
A 50 years old female patient came with complaints of acute onset of breathlessness and chest pain for past one week. There was no history of cough, syncope and fever. Her vitals and other lab investigation parameters were within normal limits. X- ray showed mild cardiomegaly. Echocardiography showed large left atrial (LA) mass measuring 40x25mm seen protruding into LV cavity during diastole probably attached to interatrial septum.
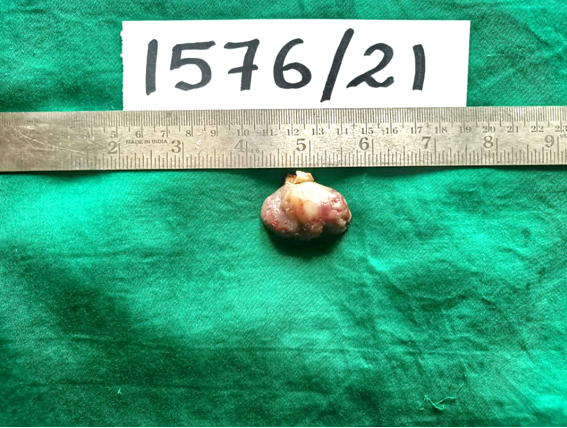
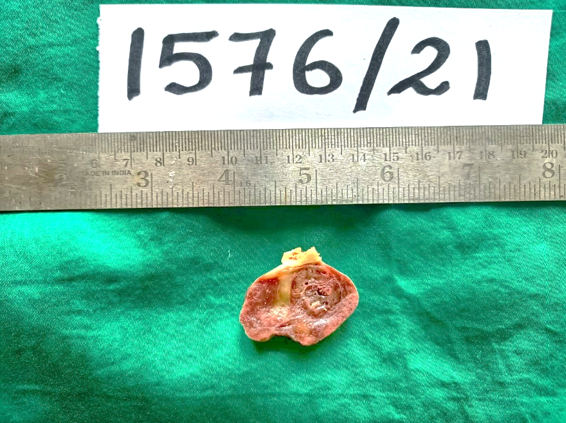
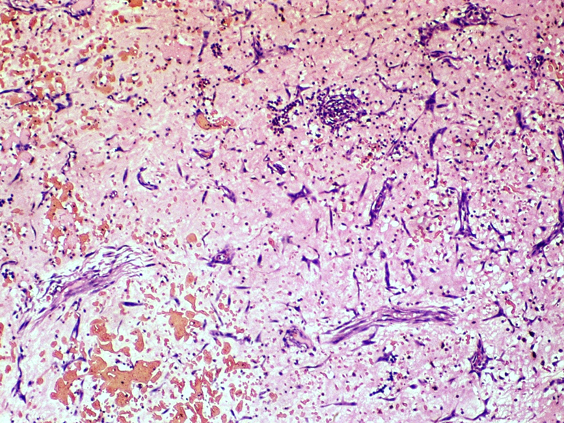
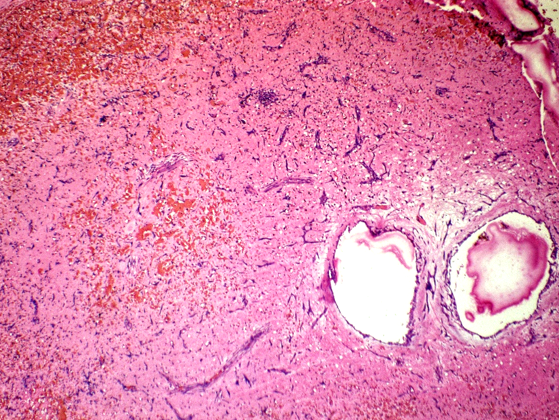
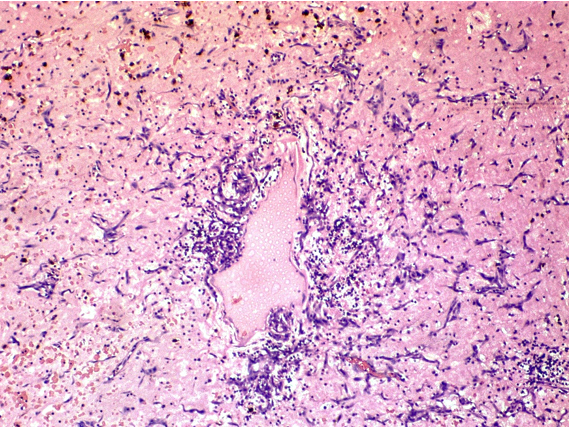
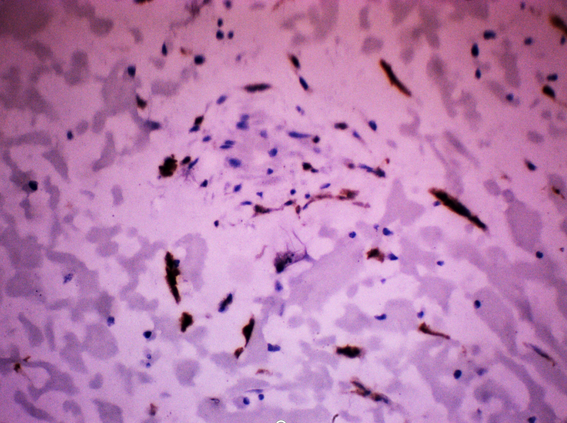
Excision of LA mass was done and was received as grey brown nodular mass measuring 3.8x2.5x2cm. Surface appeared smooth and glistening. Cut surface showed grey brown myxoid areas. Microscopic examination showed focal myocardial tissue with a neoplasm composed of stellate myxoma cells scattered singly, groups and in tiny cystic spaces. Cells had moderate amount of cytoplasm with round to oval nucleus embedded in a myxoid stroma. Vasoformative rings were seen. Matrix showed areas of haemorrhage, hemosiderin pigment and inflammatory cells.
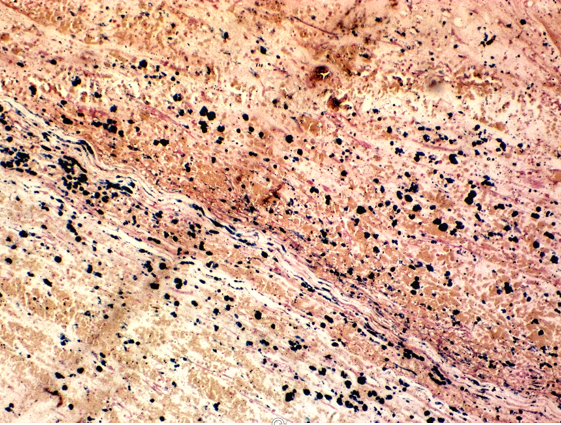
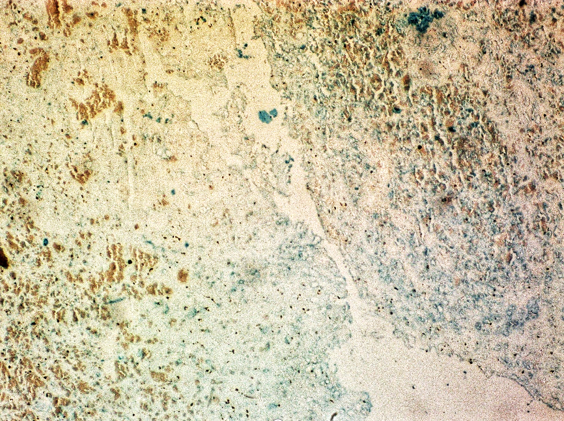
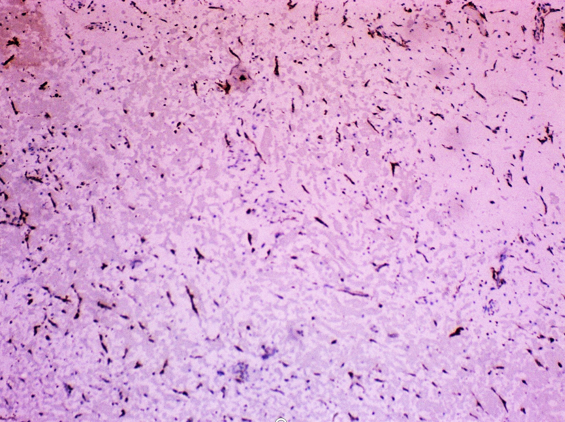
Special stains Alcian blue showed blue staining of background acid mucopolysaccaride. Perls stain showed positive staining of hemosiderin pigment macrophages. Immunohistochemistry calretinin showed positive staining in stellate cells.

Discussion
The most common primary tumour of the heart is the cardiac myxoma, which frequently occurs in the left atrium. The tumour may cause symptoms of left atrial obstruction and systemic embolization. [4] Myxomas occur most often in patients aged 30 to 70, with female predominance, and in families with a tendency to develop myxomas. [5] About 85% of myxomas occur in the left atrium, 10% in the right atrium, and 5% in the ventricles.[6] Atrial myxomas produce 3 types of clinical presentation: obstructive, constitutional, and embolic. Obstruction mimics mitral and tricuspid valve disease and occurs due to blockage of the atrioventricular valves.[7] The tumour can mimic mitral stenosis, and occasionally an early diastolic rumbling sound called ‘tumour plop’ may be heard during auscultation. Diastolic murmurs are the most common murmur heard in up to 89% of patients with cardiac myxoma.[8] Echocardiography shows a nonhomogeneous mass almost filling the left atrium completely and prolapsing through the mitral valve into the left ventricle during diastole.[9] The origin can be explained through different theories. Myxomas in recent molecular characterization has revealed protein expression profile similar to those seen in endocardial mesenchymal transformation of endocardial cushion. Less than 10% can be associated with Carney complex which is autosomal dominant disorder characterized by constellation of myxomas, endocrinopathy and spotty skin pigmentation.[10]
On gross examination, the tumours has a broad base, and most have pedicles and soft, gelatinous, and very friable on cut surface. They are smooth and glistening or have multiple papillary, villous, finger-like projections. Extremely calcified myxomas have been referred to “petrified” myxoma.[11]
Histopathological examination shows a lobulated polypoidal mass covered by endothelium and composed of abundant loose myxoid stroma with scattered round, polygonal and stellate cells with dense irregular nuclei and occasional vascular structures consisting of capillary-like spaces containing red blood cells.[12] Usually no mitotic figures, necrosis and polymorphism will be seen. Hemosiderin-Laden macrophages is commonly seen.[13] Perls stain showed hemosiderin pigment deposition and Gamna Gandy bodies. Alcian blue PAS stain demonstrated mucin positivity.[14] The myxoma cells are also been reported to be reactive with S-100 protein, calretinin, vimentin, desmin, smooth muscle myosin, CD56, α1 antitrypsin and α 1antichymotrypsin. Calretinin reactivity within myxoma cells can be particularly useful in differentiating myxoma from other entities, particularly fibroblastic lesions.[15]
Surgical resection is the treatment of choice for atrial myxoma with a low postoperative risk. It is usually curative with an excellent long-term prognosis. However, incomplete resection resulted in a recurrence rate of 1–5%. Recurrence beyond 4 years after surgery rarely happens.
Source of Funding
No financial support was received for the work within this manuscript.
Conflicts of Interest
There are no conflicts of interest.
References
- R Cohen, G Singh, D Mena, CA Garcia, P Loarte, B Mirrer. Atrial Myxoma: A Case Presentation and Review. Cardiol Res 2012. [Google Scholar]
- L Pinede, P Duhaut, R Loire. Clinical Presentation of Left Atrial Cardiac Myxoma. Med 2001. [Google Scholar] [Crossref]
- JJ Maleszewski, BT Larsen, NS Kip, MC Castonguay, WD Edwards, JA Carney. PRKAR1A in the Development of Cardiac Myxoma. Am J Surg Pathol 2014. [Google Scholar] [Crossref]
- KC Goswami, S Shrivastava, VK Bahl, A Saxena, SC Manchanda, HS Wasir. Cardiac myxomas: Clinical and echocardiographic profile. Int J Cardiol 1998. [Google Scholar] [Crossref]
- K. Yu, Y. Liu, H. Wang, S. Hu, C. Long. Epidemiological and pathological characteristics of cardiac tumors: a clinical study of 242 cases. Interact Cardio Vascular Thoracic Surg 2007. [Google Scholar] [Crossref]
- HD Tazelaar, TJ Locke, CG McGregor. Pathology of Surgically Excised Primary Cardiac Tumors. Mayo Clin Proceed 1992. [Google Scholar] [Crossref]
- M Demir, O Md, MD Akpinar, E Acarturk, F Md. Atrial Myxoma: An Unusual Cause of Myocardial Infarction. Texas Heart Inst J 2005. [Google Scholar]
- S K Aggarwal, R Barik, T C Sarma. Clinical presentation and investigation findings in cardiac myxomas: new insights from the developing world. Am Heart J 2007. [Google Scholar]
- S Schiele, SJ Maurer, CP Salvador, K Vitanova, G Weirich, C Meierhofer. Circulation: Cardiovascular Imaging. 2019. [Google Scholar]
- . WHO classification of tumours of lung, pleura, thymus and heart. 4th Edn. Lyon France: International agency for research on cancer 2015. [Google Scholar]
- L Yu-Jun, H Liu, L Ning-Ning, J Zhao, X Xiao-Ming. Clinicopathologic analysis of cardiac myxomas: Seven years’ experience with 61 patients. J od thoracic Dis 2012. [Google Scholar]
- H A Ngow, W M N Wan Khairina. Atrial myxoma: histological confirmation. Heart Asia 2011. [Google Scholar]
- MS Anvari, MA Boroumand, A Karimi, K Abbasi, H Ahmadi, M Marzban. Histopathologic and Clinical Characterization of Atrial Myxoma: A Review of 19 Cases. Lab Med 2009. [Google Scholar] [Crossref]
- E Divya, R Rukhmangadha, A Patnayak, A Chandra, Hari Krishna P Murthy. Glandular myxoma of left atrium: An uncommon tumor. Heart India 2016. [Google Scholar]
- O Hernández-Bringas, C Ortiz-Hidalgo. Características histopatológicas e inmunohistoquímicas de los mixomas cardiacos. Archivos Cardiologia de Mexico 2013. [Google Scholar] [Crossref]