- Visibility 155 Views
- Downloads 12 Downloads
- DOI 10.18231/j.jdpo.2021.019
-
CrossMark

Role of exfoliative cytology in diagnosis of oral lesions: With special reference to rule out malignancy
Introduction
Exfoliative Cytology has been broadly confirmed as a tool in the early detection of malignancy and has taken its appropriate position besides the other known branches of hospital diagnostic services.[1] Any laboratory method must meet three principle requirements, to achieve wide acceptance and these are (a) the method should be easy to perform, (b) it should give minimal discomfort and disadvantage to the patient (c) it must provide exact outcome. The method of cyto-diagnosis meets these three requirements very well and that is why it has gained popularity with in such a short period of time since its introduction by George N. Papanicolaou. [2] Clinical cytology, in the hands of well trained personnel now possess a sensitivity of 92 to 100% while its specificity has risen to somewhere between 97 to 100 % (Nils G. Stromby,1999).[2] It has been reported that majority of the carcinomas of the oral cavity are of well differentiated squamous cell type. In these type of malignant cases the malignant cells have a characteristic cytologic appearance and are quite easily recognized.[3] This guarantee that cyto-diagnosis is likely to yield a high degree of accuracy in cases of oral malignancies, cytological diagnosis is still in its infancy for the recognition of premalignant lesion in various areas of the human body. From the results achieved by workers like Sandler it seems there is great promise in its use in oral premalignant lesions and in-situ carcinomas.[3], [4], [5], [6], [7] the oral cancers as in other regions of the body freely exfoliate and, therefore, smears prepared from regions that harbor a cancer are usually rich in number with variety of exfoliated malignant cells.[8] Silverman, Becks and Farber (1977) have suggested that cytological technique, being simple and non-invasive procedure, has the advantage of doing away with many undesirable features of a biopsy and that offers a easy yet reliable method of great predictability in cancer detection programme. [9] It was with this view that the present work had been undertaken. The present research has been taken to find out whether cancer can be detected in its preinvasive stage by use of exfoliative cytology, in addition an effort has been made to explore the possibility of using this technique in detection of other oral pre-malignant lesions.
|
Age group |
Normal |
Leukoplakia |
Oral submucous fibrosis |
Mucosal hyperemia |
Traumatic ulcer |
Granular mucosa |
Carcinoma |
|
20-30 |
M = 2(8%) F = 0 T = 2 (8% |
M = 3(6.38%) F = 1(2.12%) T = 4(8.5%) |
M = 0F= 1(16.7%)T= 1(16.7%) |
M = 0 F = 0 T = 0 |
M = 0 F = 0 T = 0 |
M = 0 F = 0 T = 0 |
M = 0 F = 0 T = 0 |
|
31-40 |
M = 1(4%) F = 2(8%) T = 3 (12%) |
M= 10(21.2%) F = 1(2.12%) T = 11(23.4%) |
M=1(16.7%) F=2(33.3%) T=3(50%) |
M = 0 F = 0 T = 0 |
M = 0 F = 0 T = 0 |
M=1(100%) F = 0 T=1(100%) |
M=3(15%) F =2(10%) T =5(25%) |
|
41-50 |
M = 6(24%) F = 6 (24%) T=12 (48%) |
M= 14(29.7%) F = 4(8.5%) T = 18(38.2%) |
M = 0 F= 1(16.7%) T= 1(16.7%) |
M = 0 F = 0 T = 0 |
M = 0 F=1(100%) T=1(100%) |
M = 0 F = 0 T = 0 |
M=4(20%) F =2(10%) T =6(30%) |
|
51-60 |
M = 4(16%) F = 4(16%) T = 8(32%) |
M= 8(17.02%)F = 1(2.12%)T = 9(19.14%) |
M=1(16.7%) F= 0 T= 1(16.7%) |
M=1(50%) F=1(50%) T=2(100%) |
M = 0 F = 0 T = 0 |
M = 0 F = 0 T = 0 |
M=4(20%) F =2(10%) T =6(30%) |
|
61-70 |
M = 0 F = 0 T = 0 |
M = 3(6.38%) F = 0 T = 3(6.38%) |
M = 0F = 0T = 0 |
M = 0 F = 0 T = 0 |
M = 0F = 0T = 0 |
M = 0 F = 0 T = 0 |
M=3(15%) F = 0 T =3(15% |
|
71-80 |
M = 0 F = 0 T = 0 |
M = 2(4.25%) F = 0 T = 2(4.25% |
M = 0 F = 0 T = 0 |
M = 0 F = 0 T = 0 |
M = 0 F = 0 T = 0 |
M = 0 F = 0 T = 0 |
M = 0 F = 0 T = 0 |
|
Total 102 |
N =25 |
N =47 |
N =6 |
2 |
1 |
N=1 |
38 |
|
Mean age |
45.2 |
47.5 |
38.3 |
55 |
50 |
38 |
46.06 |
Materials and Methods
The present study was carried out over a period, from August 2019 to April 2020. The material for our study was collected from patients attending the outpatient Department of the Private Hospital including the E.N.T. and surgery department of a dispensary as well as cancer research institute Delhi for various complaints pertaining to oral cavity. Informed expressed consent was taken from all patients before including them in study. Ethical Committee approval was also taken out before starting study. In every case a detailed general oral examination was done and positive findings along with a brief clinical history were noted down most of the cases required no prior preparation. Some of the cases were found to be covered with debris or slough, surfaces of such lesions were first cleaned by wiping with a piece of gauge moistened in normal saline solution and then the scraping was done. The cases which were highly keratinized in those lesions the keratinized surface was removed by scraping it with a wooden spatula. In case of the lip lesions, the involved areas were first soaked with a piece of wet gauge for about 15 minutes before taking the scraped specimen. Carefully labelled slide was held between the left thumb and the fore finger, the angle of the mouth was drawn laterally with the help of left little finger, a wooden tongue depressor which had previously been soaked in tap water was held in the right hand and with its help the entire surface of the lesion was scraped vigorously using the edge of the wet tongue depressor several times but mostly in one direction. Scraping thus picked up on the edge of the tongue depressor were spread evenly and rapidly over the glass slide and the slide was immediately fixed with spray fixative given in Rapid PAP kit. Two smears were always prepared from each patient. The smears were allowed to air dry. In the present study, prepared smears were stained by Rapid PAP kit. The slides were mounted with cover slip using a drop of D.P.X. Mountant.
After screening cytologic smears were classified according to Papanicolaou’s (1960)[2] classification: Class I (Normal) – Only Normal cells were observed
Class II (atypical) – Presence of minor atypia, but no evidence of malignancy.
Class III (Intermediate) – The cells display wide atypia that may be suggestive of malignancy, but they are not clear cut cancer and represent precancerous lesions or in situ carcinoma.
Class IV (Suggestive of cancer) – A few epithelial cells with malignant characteristics or cells with borderline characteristics.
Class V – Positive cancer cells, that are obviously malignant.[2]
Result
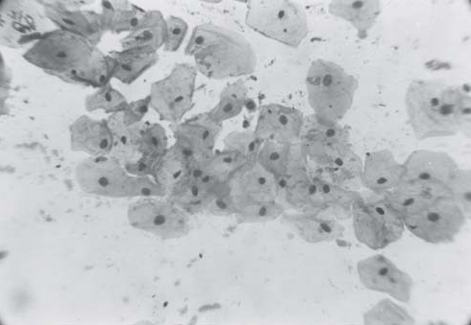
A total of 204 oral mucosal smear from 102 patients were taken, in which 25 were normal group. The normal group was taken as control. The control group consists of people with out any complain, clinical examination the oral mucosa appeared absolutely normal. Cases with history of tobacco chewing and smoking were not included in the control group. ([Table 1]) In our study the maximum age group of Leukoplakia was 31-40 years observed in 61.7% cases with mean age of 47.5 and 85% cases were male. In Leukoplakia 97.8% cases were either tobacco chewer or smokers and 12.7% patients came with complaint directly related to the leukoplakic patch while remaining were unaware with the problem. 87.2% the most common site of involvement was buccal mucosa. ([Table 2]) No malignant cells were evident on any smear of Leukoplakia. Anucleated squames were present in 53% cases. In 38% Leukoplakia cases, mild degree acidophilia and moderate acidophilia in 36% cases was seen. Karyorrhexis 25%, prominent nuclear membrane 11%, prominent nucleoli 6% and rarification of nuclei 4% cases were observed. ([Table 4]) 06 cases of submucous fibrosis were included in study. 50% were age group of 31-40 years (mean age 38.3 years) and 66.7% female. All cases were with complaint of restricted movement of lower jaw and inability to open mouth completely. No history of tobacco or betel nut chewing among female patients. Cytologically smear showed 66% rarification of nuclei, 50% irregular maturation of cytoplasm, and 50% mild atypia cases. No malignancy was evident in the osmf cases.
|
Symptoms |
No of cases |
|
Recurrent ulcer |
3(6.28) |
|
Excessive salivation |
2 (4.25) |
|
Itching in oral cavity |
1 (2.21%) |
|
Burning mouth |
1 (2.21%) |
|
No symptoms |
1 (2.21%) |
|
Site of involvement of mouth in 20 cases |
39(82.9%) |
|
Clinically suspected to be malignancy |
N =47 |
Location No of cases
|
Location |
No of cases |
|
Buccal mucosa |
7(35%) |
|
Tongue |
5(25%) |
|
Alveolar margin |
3(15%) |
|
Tonsil |
2(10%) |
|
Base of tongue and tonsil |
1(5%) |
|
Alveolar margin and cheek |
1(5%) |
|
Lip |
1(5%) |
|
Anucleated squames |
53% cases |
|
mild degree acidophilia |
38% |
|
moderate acidophilia |
36% |
|
Karyorrhexis |
25% |
|
Prominent nuclear membrane |
11% |
|
prominent nucleol |
06% |
|
rarificationof nuclei |
04% |
|
Rarification of nuclei |
66% cases |
|
Irregular maturation of cytoplasm |
50% |
|
Mild atypia |
50% |
|
Malignancy |
0% |
In our study mucosal hyperemia (erythema) 02 cases were included. 01 case was male patient having a history of chronic smoking also there was presence of erythematous patche on the palate. The second case was female patient with no history of tobacco chewing. Smears from these lesions revealed increased number of superficial cells and a fair number of polymorphonuclear cells.
One female patient present with a chronic traumatic ulcer on her upper lip was also studied. Smears revealed mild degree of dyskaryosis in epithelial cells. 01 male patient having granular buccal mucosa was also included in the present study, smears prepared from mucosal surface did not reveal any significant abnormality.
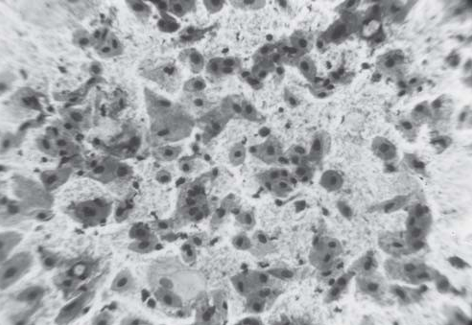
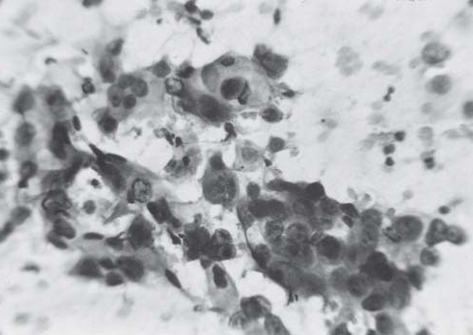
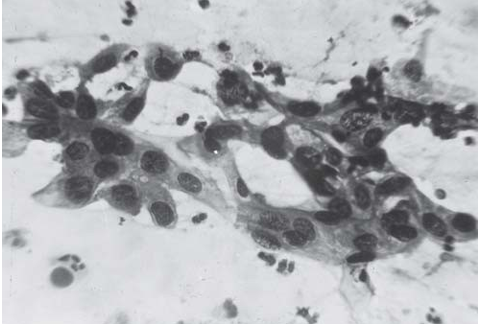
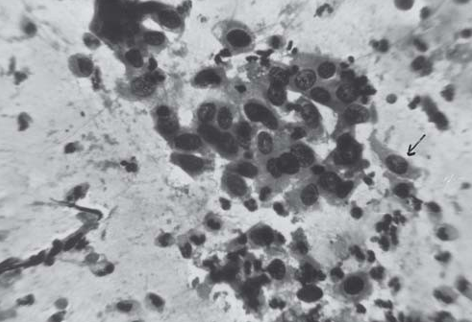
In this study we found twenty cases of the cancer with maximum age incidence 41-60 years (mean age 46 years) and 70% were male and 100% cases with the history of tobacco chewing or smoking. The most common sites were cheek and tongue with incidence of 60%. The smear showed inflammatory cells in 100%, malignant cells in 75% cases either in groups or in singles. The third type of cells (cells having stand and clumps of nuclear chromatin, unevenly deposited at nuclear borders, irregular but well defined cytoplasmic borders and increased nuclear cytoplasmic ratio) were observed in 60% cases. The undifferentiated cells (cells in whom cellular borders are absent, nuclei are hyperchromatic, irregular in size and shape, chromatin arrangement in abnormal and nuclear borders are very sharp) were observed in 37% cases. Tadpole cells were least observed only in 5% cases.
Out of 20 clinically cancer suspected individuals, 75% were positive for cancer, 10% were suspicious for cancer and remaining 15% were given as negative for cancer.
Discussion
In our study the maximum age incidence in 61.7% cases of Leukoplakia was 31-40 years. Tieche (1965) observed 80-90% cases were above 40 years. [10] 85% Majority cases were male in present study. In (1961) Shafer and Waldron made similar observation in 321 cases among these cases 70% were males. [10], [11] Buccal mucosa and alveolar mucosa were most common site of involvement of Leukoplakia by Tieche (1965) [10] similar observation 87.2% were obtained in our study . On microscopy, 74% of cases of Leukoplakia revealed predominant acidophilic character of cytoplasm in exfoliated cells and 51% of cases showed pyknotic nuclei, which is similar to observation by (1954) Wahi and Gupta approximately 75% of exfoliated superficial cells. [12] Another significant finding was Anucleated squames in present study it was 53.2%, while Montgomery and Von Hamm (1951A) were so impressed with the findings of Anucleated squames that they thought it to be almost diagnostic of the leukoplakic lesions. [13] In case of advanced Leukoplakia, varying degree of nuclear atypia of exfoliated cells in smear were observed. [14], [15] In the present study 11% cases of leukoplakia, revealed moderate degree of nuclear atypia. 50% submucous fibrosis cases were in age group of 31-40 years and 66.7% were female in the present study while in previous studies this was similar. In (1954) Sirsat and Khanolkar in their study of 40 cases reported 18 (45%) female and 22 (55%) male and Joshi et al (1953) cited by Sirsat and Khanolkar (1957), out of 41 cases 19 (46.3%) were male and 22 (53.7%) were females.[16]
An interesting finding in the smears from these areas was finding of rarified nuclei in 66% of cases. In 1955 Wahi and Kehar[15] have reported 68-82% of rarified nuclei in cyanophilic cells. In (1956) Peters and Rysinghani also have similar observation. They considered it, significant finding as far as the cytological diagnosis of oral submucous fibrosis was concerned.[14] Use of exfoliative cytology and cytoanalysis is a useful early diagnostic method for epithelial atypia and for oral lesion. [17] There were 20 cases in this series, which were suspected to be of cancer on clinical examination. 70% patient were male and 60% in the age group of 41-60 years, with mean age of 46 years. In 1965 Tieche reported average age incidence was 55 years and 80- 85% were male.[10] That may be because of excessive tobacco chewing and smoking in India. The third type of cells were the most commonly observed malignant cells in the present study, it was seen in 60% of cases. The undifferentiated cells were comparatively less frequently observed (33%). Tadpole cells were the least commonly encountered cells and seen only in one case. King (1962) found fiber cells and tadpole cells only in 2 cases of his series. "Third type" differentiated cells were commonly seen.[18] Cawson (1960) also found tadpole cell less common in smears of oral carcinoma (only in 1 case).[19] Abnormally large nucleoli were seen in 66% of smears from patient suffering from oral carcinoma in our study. Montgomery found prominent nucleoli from 86% of such smears.[20] Prominent nuclei were considered to be a common observation in smears from cases of carcinoma of mouth by many workers.[8], [9], [19], [21]
Conclusion
Cytological diagnosis is essential for the diagnosis of oral lesions, especially in distinguishing benign lesions from malignant ones, it is important for treatment as well as for clinical and epidemiological research including the study of prognosis. So far as diagnosis of presence or absence of malignancy in a lesion is concerned with high accuracy rate in diagnosing oral cancer cytology is considered as a reliable diagnostic tool. This procedure is not intended to replace tissue biopsy, but it is a valuable supplement to tissue biopsy. Indications for its use include oral mucosal lesions, and follow up for patient with a history of either a premalignant or malignant lesion. The oral cytologic technique is easy to do and can provide help to the surgeon / physician, in cases where he/she might hesitate to perform an invasive procedure, like a biopsy.
Source of Funding
No financial support was received for the work within this manuscript.
Conflicts of Interest
There are no conflicts of interest.
References
- . American Cancer Society: Cancer Facts and Figures 2005. Atlanta, Ga: American Cancer Society, 2005. Also available online. Last accessed May 20, 2005. . [Google Scholar]
- NG Stromby. Experience with buccal smears in the general cytopathology laboratory. Cancer 1999. [Google Scholar]
- WAD Anderson. Pathology. 10th Edn. 1996. [Google Scholar]
- H C Sandler. The detection of early cancer of the mouth by exfoliative cytology. Acta Cytol 1961. [Google Scholar]
- HC Sandler. Oral exfoliative cytology. Veterans Administration Co-operative study. 1962. [Google Scholar]
- H C Sandler. Veterans Administration Co-operative study of oral exfoliative cytology. Acta Cytol 1963. [Google Scholar]
- HC Sandler. Reliability of Oral Exfoliative Cytology for Detection of Oral Cancer. J Amer Dent Ass 1964. [Google Scholar] [Crossref]
- H Peters. Cytologic smears from the mouth: Cellular changes in disease and after radiation. Am J Clin Path 1958. [Google Scholar]
- S Silverman, H Becks, S M Farber. The diagnostic value of intra-oral cytology. J Dent Res 1977. [Google Scholar]
- R W Tiecke. Oral Pathology, New York. The Blakiston Division. 1965. [Google Scholar]
- WG Shafer, MK Hine, BM Levy. A text book of oral pathology. 2nd Edn. 1963. [Google Scholar]
- PN Wahi, K Gupta. Exfoliative cytology in diagnosis of carcinoma of oral cavity. J Ind Med Ass 1954. [Google Scholar]
- PW Montgomery, EV Haam. A Study of the Exfoliative Cytology of Oral Leucoplakia. J Dent Res 1951. [Google Scholar] [Crossref]
- H Peters, K Rysinghani. The cytologic interpretation of mouth smears. J Ind Med Ass 1956. [Google Scholar]
- P N Wahi, U Kehar. Morphological and cytochemical studies of precancerous lesions of oral cavity. Acta Cytol 1966. [Google Scholar]
- SM Sirsat, VR Khanolkar. Histochemical and electron microscopic study of submucous fibrosis of the palate. Ind J Path & Bact 1957. [Google Scholar]
- HG Ahmed, A M Idris, S O Ibrahim. Study of oral epithelial atypia among Sudanese tobacco users by exfoliative cytology. Anticancer Res 2003. [Google Scholar]
- OH King. The cytology of common and uncommon oral malignancies. Acta Cytol 1962. [Google Scholar]
- R A Cawson. The cytological smear in diagnosis of oral cancer. Br Dent J 1960. [Google Scholar]
- PW Montgomery. A Study of Exfoliative Cytology of Normal Human Oral Mucosa. J Dent Res 1951. [Google Scholar] [Crossref]
- HC Sandler, SS Stahl. Exfoliative cytology; a diagnostic aid in the detection of oral neoplasms. J Oral Surg 1958. [Google Scholar]