Introduction
Breast cancer is a commonest malignancy of women globally.1 The incidence of breast carcinoma in worldwide is 10.4%, developed countries have higher incidence.2, 3 It is the second most common type of non-skin malignancy (after carcinoma of lung) and fifth most common cause of cancer death.2 A palpable breast lump is a common diagnostic dilemma to surgeons, so it is important to differentiate a benign from malignant breast lesions for surgical pathologist.1, 4
FNAC (fine needle aspiration cytology) is simple, reliable, cost effective diagnostic tool with excellent patient acceptance.5 It helps in differentiating malignant from benign breast lesions, and it plays an important role in Triple test along with clinical and mammography examination in assessment of breast lumps.6
Mammography is other screening diagnostic modality for a breast lump which is routinely used method with simple, low cost with high accuracy.3 Benign breast lesions are round to oval in shape with regular, linear margin, homogenous echo texture and hypoechoic. Whereas malignant breast lesions are irregular in shape with ill defined speculated margins and microcalcification present.7
Due to increase in public awareness and advancement in screening led to early detection and planning of treatment in breast carcinoma. Consequently, decreased morbidity and mortality rate particularly in younger women.2
The aim of present study is to differentiate and categories the palpable breast lumps and to study the correlation, accuracy of FNAC with Histopathology of palpable breast lumps.
Materials and Methods
One and half year retrospective study carried out from January 2019 to June 2020 in department of pathology, KBNIMS, Gulbarga. FNAC was done with 23 gauge needle following standard procedure under aseptic precautions. Slides were air dried, fixed, with ethylalcohol and stained by field, Giemsa and haematoxylin and eosin. Specimen received for histopathological study was processed and stained by H&E technique, followed by microscopic examination.
FNAC and histopathology slides were retrieved and reviewed. All the slides were observed and findings recorded. The mammography findings were retrieved and recorded. The ethical clearance was obtained from the institutional ethical committee. Statistical analysis carried out.
Results
The present study includes 125cases out of which 101 cases (80.8%) were benign and 24 cases (19.2%) were malignant. Fibroadenoma (Figure 1 A,B,C) 53 cases (52.4%) constituted the largest disease group in benign breast lesion with a maximum incidence in the third decade of life, followed by Fibrocystic disease (Figure 2A,B) 23 cases, Chronic granulomatous mastitis (Figure 3A,B) 8 cases, Benign Phylloides 5 cases, Lactating adenoma 4 cases and Atypical ductal hyperplasia 3 cases (Table 1, Table 2).
Table 1
Diagnostic table of benign and malignant lesions as per FNAC and Histopathology
Table 2
Age range among benign and malignant breast lesions
Infiltrating ductal carcinoma (Figure 4A,B)18 cases (75%) was most common malignant breast lesion, followed by Medullary carcinoma (Figure 5A,B) 2 cases, Intraductal carcinoma (Figure 6A,B) 2 cases, Mucinous carcinoma (Figure 7A,B,C) 1case and Papillary carcinoma (Figure 8A,B) 1case.
Frequency of left breast lesions were high (75%) compare to right breast lesions. There were 2 bilateral cases of benign breast lesions.
Majority of benign breast lesions were seen within the age bracket of 10 to 40 years and malignant lesions were seen within the age bracket of 30 to 70 years. The earliest malignant lesion was detected at the age of 30 years (Table 2). This suggests that breast malignancy can occur in young women.
In present study, Benign breast lesions clinically presented with freely mobile small size(2-3cm)breast lump, majority of cases without any associated symptoms, few cases had localize pain. Malignant breast lesions clinically presented as large breast lump (5-6cm) which was adherent to underlying tissue with nipple retraction, many cases had axillary lymphadenopathy.
Out of 125 cases, FNAC of 123 cases (98.4%) were correlate with histopathology. In one case of breast lump in a 38 years old female, which was diagnosed as fibrocystic disease with atypia on FNAC. On excisional biopsy of that breast lump histopathology confirmed as an infiltrating ductal carcinoma. In another case of 35years female with breast lump was diagnosed as fibroadenoma on FNAC with mild nuclear atypia with few myoepithelial cells. On excisional biopsy histopathology confirmed as infiltrating ductal carcinoma.
The statistical analyses of FNAC with respect to breast malignancy were done (Table 3). The sensitivity of FNAC was found to be 91.66%, specificity of 100%, positive predictive value (PPV) of 100% and negative predictive value (NPV) of 98%. The accuracy rate was calculated as 98.4%.
Table 3
Cyto-histological correlation of breast lesions
Out of 125 cases of breast lumps, mammography of 25 cases were retrieved. In that 23(92%) cases correlated with Histopathology. One case on mammography was reported as benign breast lesion (BIRAD 2), On FNAC it turned out as malignant, which was confirmed by histopahological examination. Second case on mammography reported as malignant (BIRAD 4), on FNAC it turned out as cellular fibroadenoma, later on excisional biopsy for histopathology confirmed as cellular fibroadenoma.
In present study, on mammography benign breast lesions showed well defined oval, hypoechoic lesions with smooth, regular margins. No associated architectural distortions. Nipple , areola complex and underlying pectoral muscles appear normal(BIRAD 1,2 AND 3)(Figure 9). Malignant lesions showed radiodense mass with irregular margins with mild increase in vascularity and tiny calcifications noted, associated with distortion of normal architecture(BIRAD 4 AND 5)(Figure 10).
The sensitivity of mammography for detecting breast malignancy was 87.5% and specificity was 94.11% with diagnostic accuracy of 92%.
Figure 1
A: Fibroadenoma smear Showing branching sheets of bland epithelial cells, admixed with myoepithelial cells (Field stain, 10X, Cytology), B: Fibroadenoma section showing both epithelial and stromal elements (HandE, 20X, Histopathology), C: Cellular fibroadenoma section showing stromal hypercellularity (10X, Histopathology)
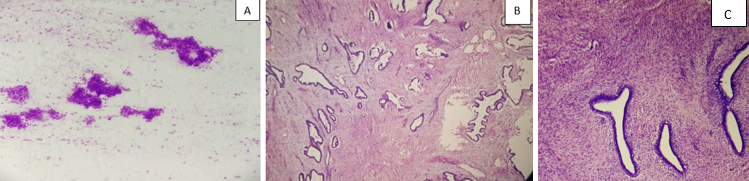
Figure 2
A: Fibrocystic Disease section showing cystically dilated glands with hyperplastic epithelium. (20X, Histopathology), B: Fibrocysic Disease smear showing Sheets of ductal epithelial cells with apocrine change (20X, Field stain, cytology)
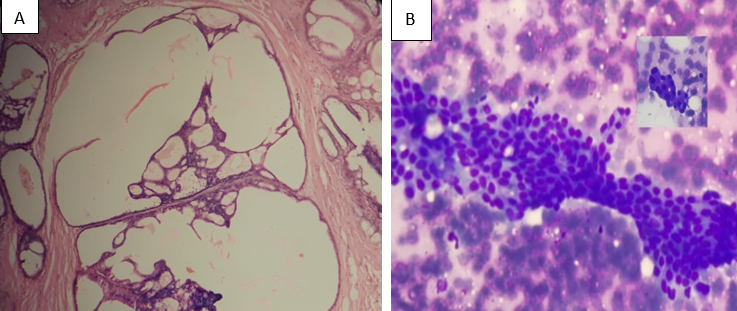
Figure 3
A: Granulomatous mastitis smear showing epithelioid cells (40X, cytology), B: Granulomatous mastitis section showing granuloma (20X, Histopathology)

Figure 4
A: Infiltrating ductal carcinoma smear showing pleomorphic tumor cells with prominent nucleoli (20X, cytology), B: Infiltrating ductal carcinoma section showing Pleomorphic tumor cells arranged in clusters (10X, Histopathology).
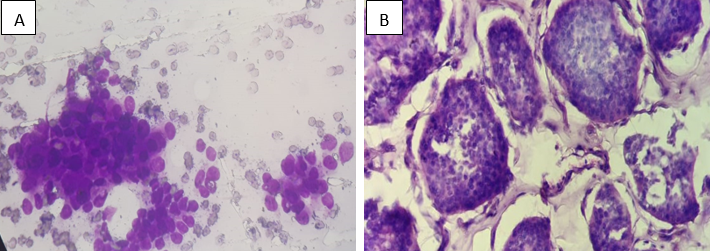
Figure 5
A: Medullary carcinoma smear showing large pleomorphic tumor cells with coarse granular nuclei with background of lymphocytes (20X, Cytology), B: Medullary carcinoma section showing Tumor cells arranged in syncytial pattern with pushing borders and surrounded by lymphocytes (20X, Histopathology)

Figure 6
A: Intraductal carcinoma smear showing Pleomorphic tumor cells arranged in clusters with clear background (10X, cytology), B: Intraductal carcinoma section showing cribriform pattern (10X, Histopathology)
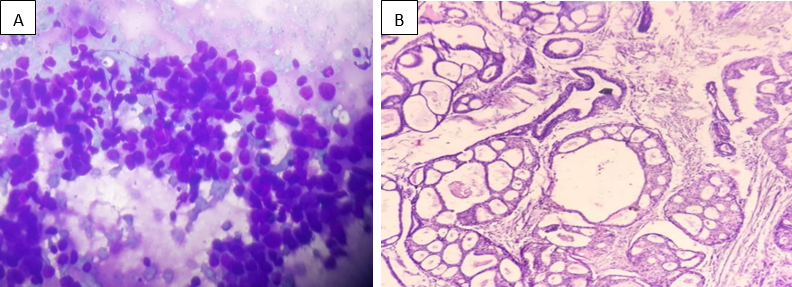
Figure 7
A: Mucinous carcinoma smear showing tumor cells with the background of mucin (20X, Cytology), B: Mucinous Carcinoma section showing Tumor cells floating in lightly staining amorphous mucin surrounded by connective tissue bands. (20X, Histology), C: Mucicarmine stain for mucin positive (red in color) (40X)
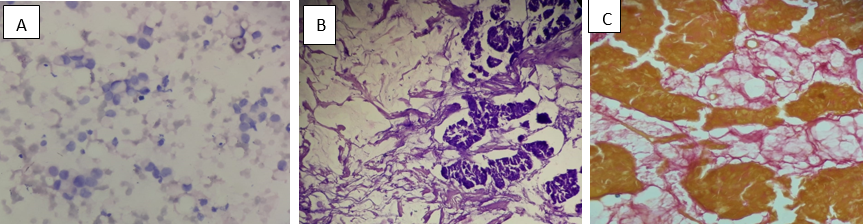
Figure 8
A: Papillary carcinoma smear showing tumor cells arranged in papillary pattern (40X, cytology), B: Papillary carcinoma section showing tumor cells arranged in papillary pattern (20X, Histopathology)
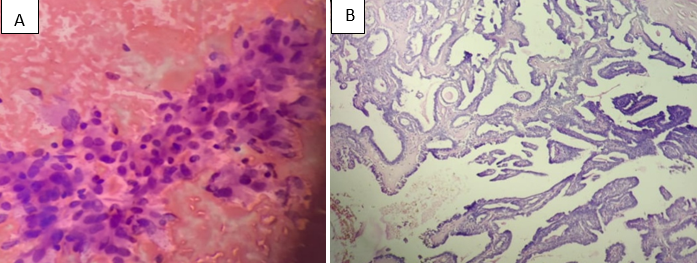


Table 4
Comparative analysis of FNAC in breast lesions by differentauthors.
|
Study |
Sensitivity |
Specificity |
PPV |
NPV |
Accuracy rate |
|
Patel A et al5 (2018) |
97.46 |
100 |
100 |
100 |
99.02 |
|
Ibikunle DE et al 4 (2017) |
99.4 |
100 |
100 |
66.7 |
- |
|
Khageshan AP et al 8 (2015) |
96.97 |
100 |
100 |
98.63 |
99.05 |
|
Sankaye SB et al 9 (2014) |
88.37 |
96.42 |
97.43 |
84.37 |
91.54 |
|
Khemka A et al 10 (2008) |
96 |
100 |
100 |
95.12 |
- |
|
Muhammed AZ et al 11 (2005) |
90.6 |
100 |
100 |
99 |
- |
|
Ishikawa T et al 12 (2007) |
86.3 |
98.2 |
97.9 |
- |
- |
|
Present study |
91.66 |
100 |
100 |
98 |
98.4 |
Discussion
The incidence of breast malignancy has increased worldwide due to advancement in screening, diagnosis and changes in life style of women.6 Early detection and screening can decrease breast carcinoma mortality around 18-29%.13
FNAC of palpable breast lumps is a well accepted and established diagnostic tool for determining the benign or malignant breast lesions with high degree of accuracy. Further this is helpful in early detection and accurate management.14
The goal of present study is to correlate the results of breast lesion on FNAC with histopathological diagnosis and to assess its diagnosic accuracy. Early screening and accurate diagnosis is very necessary for categorization of breast lesions and management.
In present study fibroadenoma was most common benign breast lesion which is in agreement with Dominguez et al,15 Tiwari,16 Qasim et al, 17 Srikanth 18 and Yalavarthi et al.19
In our study majority of benign breast lesions were seen within the age bracket of 10 to 40 years, which is in agreement with Khemka et al.10 (15-44 years) and Rocha et al20 (14-40 years). However, MacIntosh et al.21 had majority of benign cases within the age bracket 27-77 years.
In present study most common malignant breast lesion was infiltrating ductal carcinoma 18 cases (75%), similar findings were seen in Domingues et al15 and Srikanth.18
In our study malignant lesions were in the age bracket of 30-70 years, which is in agreement with other studies like Srikanth18 (31-70 years), Khemka et al10(35-84 years), MacIntosh et al21(63-79 years) and Rocha et al20 (41-75 years). This suggests that breast malignancy can occur as early as 4th decade of life.
In present study distribution of breast lesions were more in the left breast (75%) compared to right breast. Similar findings were seen by Meena et al,22 Reddy and Reddy23 and Clegg-Lamptey and Hodasi.24 However Sankaye et al9 has found equal distribution on both side and Srikant18 and Rupom et al1 has found more in right breast.
The BIRAD reporting system of mammography was introduced in 1993, since then it has become important diagnostic tool in predicting the likelihood of breast carcinoma.25 In present study sensitivity and specificity of mammography for detecting malignancy in breast lesion was 87.5% and 94.11% respectively which correlates well with Richie et al25 had sensitivity of 90.6% and specificity of 97.8% and shanibi et al26 sensitivity of 88.8%.
The present study had almost 98.4% of well correlation of cytology to histopathology which correlates well with Rupom et al, 1 and Chiemchanya et al.27 The sensitivity of 91.66% in our study is comparable with that of various authors shown in Table 4, where sensitivity ranges from 86% to 99%. In present study, there was no false positive case, hence positive predictive value (PPV) and specificity calculated as 100% which is similar to Patel A et al, 5 Ibikunle DE et al,4 Khageshan AP et al,8 Khemka A et al10 and Muhammed AZ et al.11 Sankaye SB et al9 had specificity of 96.42% and PPV of 97.43%, and Ishikawa T et al12 had specificity of 98.2% and PPV of 97.9%. Thus false positive diagnosis is relatively rare in breast FNAC.
Conclusion
The present study concludes that FNAC is a valuable diagnostic tool; provide rapid and accurate diagnosis in breast lesions and it eliminates the need of surgical procedure for the diagnosis. FNAC help us to differentiate malignant from benign breast lesions with high specificity, sensitivity and accuracy.
Furthermore, Establishment of newer diagnostic modalities like immunohistochemistry, mammography, and doppler in sonomammography may increase their accuracy. However histopathological examination remains gold standard for the diagnosis.