Introduction
Fine needle aspiration cytology (FNAC) is a simple, rapid and economical met hod to sample superficial swellings found in the head and neck region.1 The technique is performed in the OPD and is non – invasive procedure. The main goal of FNA is to determine the presence or absence of neoplasm, assure the clinical benign impression of the mass, and if malignant, to determine the type of malignancy.2 Although FNAC has been proven effective in diagnosis of solid masses of head and neck, It can be both diagnostic and therapeutic in cystic swellings.3 Its usefulness in diagnosis of cystic masses in these sites is much less certain.4
It is helpful for the diagnosis of salivary gland tumours where it can differentiate between a malignant and a benign tumour with over 90% accuracy.5
FNAC is particularly helpful in the work-up of cervical masses and nodules because biopsy of cervical swelling should be avoided unless all other diagnostic modalities have failed to establish a diagnosis.6 FNAC does not give the same architectural detail as histology but it can provide cells from the entire lesion as many passes through the lesion can be made while aspirating.7 FNA has a high diagnostic accuracy, but problems may arise, primarily affecting sensitivity of technique, especially if the aspirated mass is cystic.8
Head and neck lesions comprise of developmental, inflammatory and neoplastic conditions. Commonly se en swellings are thyroglossal cysts, dermoid cysts, lymphangioma, haemangioma, lymphadenitis, sialadenitis, lipomas and neoplastic pathologies.9 FNAC has an accuracy rate exceeding 92%.10 FNAC plays an important role in the diagnosis of metastatic disease; it not only confirms the diagnosis but also helps to determine the nature of primary tumor.11 Tuberculous lymphadenitis being common in head and neck area can be diagnosed with a sensitivity ranging from 70 to 90%.12 Salivary gland FNAC has gained wide spread acceptance with reported sensitivity and specificity for diagnosing neoplasm almost more than 90%.13 Moreover, FNAC has also been reported to be most accurate at diagnosing epithelial cysts14
Materials and Methods
This Prospective observational study was conducted in the Department of Pathology in GMCDoda.
Exclusion criteria
Lesions other than Head and Neck were excluded from the study.
The Present study was carried out on 116 patients presenting with head and neck swellings over a period of 9 months . The relevant clinical details, history regarding the swelling, local examination of the swelling were taken. Special investigations like Ultrasound, were done where required particularly for the thyroid and Salivary gland lesions in order to determine the origin and nature of lesion in the form of diffuse, Hyperechoic / Isoechoic /Hypoechoic solid lesions, BIRADS /TIRADS in case of thyroid lesions . FNAC was performed by the Pathologist in the department. Aspiration was carried out using 20ml disposable dispovan syringe with 20 -25 gauze needle attached to Franzen's aspiration handle or with the needle only . Smears were air dried and fixed in acetone free methyl alcohol, stained with the help of MGG(May -Grunwald Giemsa) stain, Romanowsky group of stains, slides were mounted with DPX mountant. One or two wet smears were fixed in 95% ethyl alcohol and stained with Papanicalaou (PAP) wherever required for the assessment of nuclear morphology particularly in case of thyroid lesions. Special stains like ZiehlNeelson (ZN) stain were used wherever required. Findings of FNAC were recorded and patients were advised non-operative treatment and follow up or biopsy and surgical intervention depending upon the pathology. The cytomorphological features of various diseases were studied. Few cases diagnosed on FNAC were correlated with histopathology.
Results
The Present study was carried out on 116 patients presenting with head and neck swellings over a period of 9 months from May 2019 to January 2020. Out of all cases maximum number of cases were found in the age group of 31-40 years I;e25 cases followed by 11-20 years I;e 22 cases. (Table 1) Males constituted 54 cases and females constituted 62 cases with male to female ratio of 0.87:1 (Table 2) Among thyroid lesions categorized by ” THE BE THESDA SYSTEM FOR REPORTING THYROID CYTOLOGY”(TBSRTC 2016):1 case was found to be non- diagnostic/unsatisfactory(TBSRTC CAT- I),14 cases were diagnosed as benign with 9 cases as colloid nodules, 5 cases as Hashimottos thyroiditis (TBSRTC CAT-II) (Figure 1), 3 cases as Atypia of undetermined significance(AUS)(TBSRTC CAT-III), 1 case as Follicular neoplasm (TBSRTC CAT IV) (Figure 2), 1 case as Suspicious of papillary thyroid carcinoma(TBSRTC CAT V), 1 case as Papillary carcinoma thyroid (TBSRTC CAT VI)(Figure 3 ), 1 case as Anaplastic thyroid carcinoma(TBSRTC CAT VI) .(Table 3) and 1 case as thyroglossal cyst.
Among the total 41 lymphnode lesions of head and neck:23 cases were diagnosed as Non – specific reactive lymphadenitis (Figure 4), 13 cases as Chronic granulomatous lymphadenitis (Figure 5), 2 as Acute suppurative lymphadenitis, 2 cases as NHL/SLL and 1 case as Metastatic deposits of PD SCC (Figure 6).
Among the total 6 cases of salivary gland lesions :1case was diagnosed as Benign salivary gland cyst,1 as acute infective sialadenitis, 1 as Chronic infective Sialadenitis, 2 cases as Pleomorphic adenoma (Figure 7) and 1 case as Mucoepidermoid carcinoma (Figure 8).
Among the total 46 cases of Subcutaneous/cutaneous lesions of head and neck: 18 cases were diagnosed as non-neoplastic and 28 cases were diagnosed as Neoplastic. Among 18 non-neoplastic cases; 9 cases were diagnosed as abscess and 9 cases were diagnosed as Epidermal Inclusion cysts (EIC). Among 28 cases diagnosed as Neoplastic, all cases were found to be benign in natureof which19 cases were Lipomas, 3 as benign vascular lesions, 3 as benign adnexal lesions, 2 as Benign fibrous histiocytomas (BFH), 1 as benign spindle cell lesion and 1 case as benign lymphoepithelial lesion. No malignant case was diagnosed.
Table 1
| Age in years | Number of cases | Percentage |
| 0-10 | 16 | 13.7% |
| 11-20 | 22 | 18.96% |
| 21-30 | 21 | 18.10% |
| 31-40 | 25 | 21.55% |
| 41-50 | 20 | 17.24% |
| 51-60 | 9 | 7.75% |
| >60 | 3 | 2.58% |
| Total | 116 | 100% |
Age wise distribution of cases (n=116)
Table 2
| Males | Percentage | Females | Percentage | Total | Percentage |
| 54 | 46.55% | 62 | 53.44% | 116 | 100% |
Gender wise distribution of cases(n=116)
Table 3
FNAC diagnosis of thyroid lesions(n=23)/TBSRTC category
Table 4
| Diagnosis | Non –specific reactive lymphadenitis | Chronic granulomatous lymphadenitis | Acute suppurative lymphadenitis | Nhl/sll | Metastatic deposits of pd scc |
| Number of Cases | 23 | 13 | 2 | 2 | 1 |
FNAC diagnosis of lymphnode lesions of head and neck(n=41)
Table 5
| Diagnosis | Number of cases |
| Benign salivary gland cyst | 1 |
| Acute infective sialadenitis | 1 |
| Chronic infective sialadenitis | 1 |
| Pleomorphic adenoma | 2 |
| Mucoepidermoid carcinoma | 1 |
FNAC diagnosis of salivary gland lesions(n=6)
Table 6
FNAC diagnosis of subcutaneous /cutaneous lesions of head and neck region(n=46)
Figure 1
1: Photomic rograph showing thyroid follicles encroached by lymphoid cells against a colloid free bloody background( Hashimottos thyroiditis).
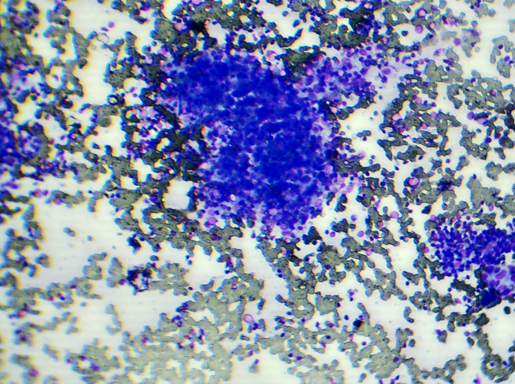
Figure 2
Photomicrograph showing follicular cells formingmicro follicles against a colloid free bloody background(Follicular Neoplasm).

Figure 3
Photomicrograph showing Tumour cells arranged inpapillaewith blunt edges withfibrovascular cores and dispersedindividually showing overcrowding, nuclear grooves and at places Intranuclearcytoplasmic inclusions(INCIS) against a background of blood mixed thick chewingum like colloid seenin other parts of the smear(Papillary thyroid carcinoma).

Figure 4
Photomicrographshowing polymorphic population of lymphoid cells with tingiblebody macrophages.(Reactive Node)

Figure 5
Photomicrograph showing epithelioid cellsinterspersed with lymphoid cells forminglarge granuloma in lymphnode(Tuberculosis)

Figure 6
Photomicrographshowing tumour cells arranged in clusters and dispersed individually havinghigh N/C ratio.( Mets PD SCC to lymphnode)



Discussion
The Present study was carried out on 116 patients presenting with head and neck swellings over a period of 9 months from May 2019 to January 2020. Out of all cases maximum number of cases were found in the age group of 31-40 years i;e25 cases followed by 11-20 years I;e 22 cases. This shows that head and neck swellings are seen mostly in the age group of 31-40 years followed by 11-20 years. Among gender distribution maximum number of cases were females. Female gender was a slightly more affected in current study and was in concordance with the study done by Dr.NaziaTabassum et al.15 Among thyroid lesions Maximum cases were diagnosed as benign (TBSRTC CAT-II) in the form of colloid nodules and Hashimottos thyroiditis. This could be due to Iodine deficiency in this region or due to Autoimmune etiology in Hashimottoscases. This shows that Neoplasm are less likely seen in this region.
Among lymph node lesions,maximum were diagnosed as Non-specific reactive lymphadenitis that too in childhood age group followed by Chronic granulomatous lymphadenitis in young population. This study is in concordance with the study done by Dr. NaziaTabassum et al.15 Among the total 6 cases of salivary gland lesions :1case was diagnosed as Benign salivary gland cyst,1 as acute infective sialadenitis, 1 as Chronic infective Sialadenitis, 2 cases as Pleomorphic adenoma and 1 case as Mucoepidermoid carcinoma. From our study this could not be interpreted as which type of diagnosis is more common because this study was done over short period of time and need further studies to be done in more number of patients.
Among the total 46 cases of Subcutaneous/cutaneous lesions of head and neck: 18 cases were diagnosed as non-neoplastic and 28 cases were diagnosed as Neoplastic. Among 18 non-neoplastic cases; 9 cases were diagnosed as abscess and 9 cases were diagnosed as Epidermal Inclusion cysts (EIC).Among 28 cases of Subcutaneous /Cutaneous diagnosed as Neoplastic, all cases were found to be benign in nature of which 19 cases were Lipomas,3 as benign vascular lesions, 3 as benign adnexal lesions,2 as Benign fibrous histiocytomas (BFH), 1 as benign spindle cell lesion and 1 cases as benign lymphoepithelial lesion. NO malignant cases was diagnosed. This shows that subcutaneous /cutaneous swellings of Head and Neck region are almost benign in this study.
Conclusion
To conclude; FNAC is considered to be the most reliable technique in the early diagnosis of various Head and Neck lesions so that proper intervention could be taken at earliest possible time in early stages and should be considered as first line investigation in the evaluation of lesions in head and neck region. It has a high degree of diagnostic yield and sensitivity to diagnose lymphnode lesions thereby obviating the need for open biopsy, thyroid lesions, salivary gland swellings and benign tumours or cystic lesions in head and neck area to plan the surgery without considering further invasive bio psy procedures preoperatively.