IP Journal of Diagnostic Pathology and Oncology
Official Publication of Khyati Education and Research Foundation
Official Publication of Khyati Education and Research Foundation
Author Details :
Volume : 4, Issue : 1, Year : 2019
Article Page : 54-57
https://doi.org/10.18231/2581-3706.2019.0010

Abstract
Introduction: Salivary gland neoplasms are known for their varied histopathological findings among individual neoplasm and difficulty in predicting the prognosis. Since benign tumors are more common in major salivary gland in particular the parotid, proper diagnosis of malignant tumors with accurate staging is essential in proper treatment and clinical management of the patient.
Aims and Objectives: The present study was carried out emphasizing on diverse histopathological findings observed in salivary gland neoplasms and giving proper diagnosis for the neoplasm.
Materials and Methods: The study was carried out in Sri Siddhartha Medical College for duration of 2 years from May 2016 to May 2018. A total of 63 cases of salivary gland neoplasms were subjected for the present study after obtaining proper consent
Results: The cases were categorized as benign and malignant. Out of total 63 cases, 41 were benign and the remaining 22 were malignant. Most commonly involved salivary gland was parotid. Pleomorphic adenoma was the most common neoplasm among benign category and Mucoepidermoid carcinoma among malignant category.
Conclusion: Salivary gland neoplasms exhibits diverse histopathological findings. A detailed histopathological examination is necessary for the proper diagnosis and henceforth clinical management. Benign tumors are more common in major salivary glands and malignant tumors are more common in minor salivary glands. In general Pleomorphic adenoma is the most common neoplasm of salivary glands.
Keywords: Salivary gland lesions, Benign neoplasms, Malignant neoplasms.
Even with their simple morphology, the salivary glands give rise to more than 40 microscopically distinct tumors. Following the proper standard classification protocols is essential. A small number of neoplasms make up more than 90% of salivary gland tumors. Salivary gland tumors are relatively uncommon and represent less than 2% of all tumors in humans.[1]
Generally salivary neoplasms are common in adults with benign tumors occurring usually in the fourth decade and malignant ones in sixth decade.[2]In sex distribution, overall incidence of salivary gland neoplasms shows high preponderance among females.[3]
Salivary gland tumors usually arise from the ductal lining epithelium and the underlying myoepithelial cells, a few arise from acini. Classification is based on the histological aspects of these neoplasms and correlates with normal salivary gland structure. Nevertheless the histological similarity does not confirm that a certain tumor arises from the structure that it mimics.[4]
70% of all the salivary neoplasms presents in parotid gland. Most common benign tumor is pleomorphic adenoma arising commonly in parotid and the most common malignant tumor is Mucoepidermoid carcinoma which occurs mostly in parotid gland followed by minor and submandibular gland.[5]
Among the minor salivary glands the most common malignant neoplasm is Adenoid cystic carcinoma and it is known for being highly malignant and notable chances of recurrence.[6]
This prospective study was carried out to know the diverse histopathological findings of various salivary gland neoplasms.
Sources of data: All the patients with salivary gland neoplasm referred from clinical section to central lab, Sri Siddhartha Medical College were included in the present study.
A total of 63 cases of salivary gland neoplasm, which were operated and specimen received at the department of pathology were subjected for the present study. Specimens received were fixed adequately followed by standard processing and staining. Each case was studied in detail and a final diagnosis was made according to WHO classification (2010).
Inclusion criteria: Those cases of salivary gland lesions which turned out to be neoplasm on histopathological examination were included in our study.
Exclusion criteria: Those cases of salivary gland lesions which were reported as non-neoplastic on FNAC and those cases whose histopathology was non-neoplastic were excluded from the current study.
Among the 63 cases included in the present study which was carried out over a period of 2 years majority were male patients and were 45 in number and females were 18 in number.
Present study saw wide range of age distribution with youngest patient being 16 years and oldest 75 years. Benign tumors were common in the fourth decade and malignant tumors in the sixth decade (Table 1).
Table 1: Showing age wise distribution of benign and malignant neoplasms.
|
Age in Years |
16-29 |
30-49 |
50-75 |
|
Benign neoplasms |
11 |
25 |
06 |
|
Pleomorphic adenoma |
06 |
16 |
03 |
|
Warthin tumor |
03 |
07 |
02 |
|
Basal cell adenoma |
01 |
02 |
- |
|
Malignant neoplasms |
0 |
06 |
16 |
|
Mucoepidermoid carcinoma |
- |
03 |
09 |
|
Adenoid cystic carcinoma |
- |
02 |
04 |
|
Carcinoma ex pleomorphic adenoma |
- |
- |
02 |
|
Adenocarcinoma |
- |
01 |
01 |
|
Total number of patients (63 cases) |
11 |
31 |
22 |
Majority of neoplasms involved major salivary glands comprising of 73% of cases and the remaining 27% cases showed involvement of minor salivary glands.
Parotid was the most common gland subjected for FNAC and biopsy. Most common neoplasm encountered in the present study was Pleomorphic adenoma comprising of 42% of all lesions and the second most common was Mucoepidermoid carcinoma comprising of 19% of cases. Other benign neoplasms diagnosed were warthin tumor in 19% of cases, basal cell adenoma in 5% of cases. Other malignant neoplasms diagnosed were Adenoid cystic carcinoma in 10%, Carcinoma ex pleomorphic adenoma in 3% and Adenocarcinoma in 3% of cases (Table 2).
Table 2: Showing various salivary gland neoplasms reported.
|
|
Number of cases |
|
Benign neoplasm |
41 |
|
Pleomorphic adenoma |
26 |
|
Warthin tumor |
12 |
|
Basal cell adenoma |
03 |
|
Malignant neoplasms |
22 |
|
Mucoepidermoid carcinoma |
12 |
|
Adenoid cystic carcinoma |
06 |
|
Carcinoma ex pleomorphic adenoma |
02 |
|
Adenocarcinoma |
02 |
|
Total |
63 |
 |
Click here to view |
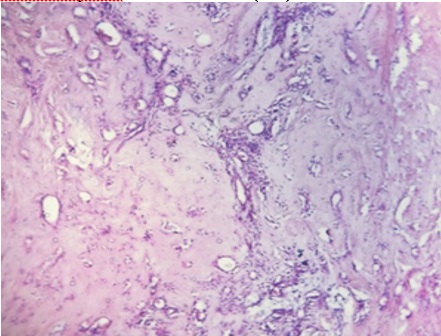
Fig. 1: HP: Microscopy of pleomorphic adenoma showing epithelial cells in cords, tubules and chondromyxoid stroma. H & E. (10x)
 |
Click here to view |
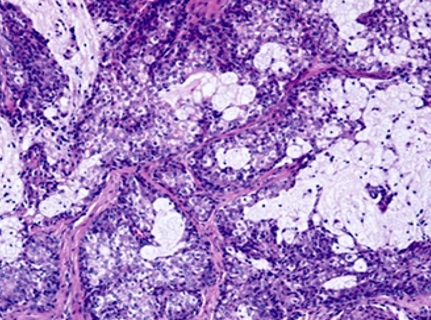
Fig. 2: HP: Microscopy of mucoepidermoid carcinoma showing intermediate cells and mucus. H & E. (40x)
 |
Click here to view |
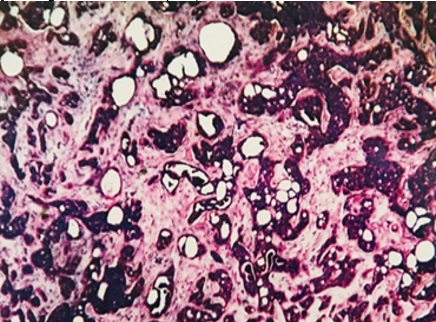
Fig. 3: HP: Microscopy of adenoid cystic carcinoma showing[1] neoplastic cells in cords, tubules and nests with cystic spaces. H & E. (10x)
Pleomorphic adenoma was the most commonly made diagnosis in the present study comprising of 26 cases. Mixed subtype was common with many showing acinar and cord like arrangement of epithelial cells. Majority of cases (21 cases) showed myxoid background with few (5 cases) showing chondroid material (Fig. 1).
The second most common diagnosis made was Mucoepidermoid carcinoma which included 12 cases. 7 cases showed predominant mucinous element and was made as Low grade MEC, remaining cases showed predominantly squamous cells and were considered intermediate in 3 cases and high grade MEC in 2 cases (Fig. 2).
Warthin tumor was reported in 12 cases. Microscopy showed lymphoid tissue and cyst like spaces lined by double layered epithelium showing foci of squamous differentiation.
Adenoid cystic carcinoma was diagnosed in 6 cases. All the cases showed incomplete capsulation. Microscopically 3 cases showed predominantly tubular pattern, 3 showed predominantly cribriform arrangement with solid areas (Fig. 3).
Basal cell adenoma was reported in 3 cases and all the cases showed basaloid cells and hyaline material.
Carcinoma ex pleomorphic adenoma was reported in 2 cases. All the cases had a history of long standing parotid swelling. Only 1 case showed features of pre-existing pleomorphic adenoma and the other case showed poorly differentiated histology.
2 cases of Adenocarcinoma was diagnosed and showed malignant glands infiltrating into the stroma.
Present study included 63 cases of salivary gland neoplasms. Out of 63 cases majority were benign with 65% of cases and the remaining 35% cases showed malignancy. Our study showed similar incidence rate comparable with other studies by Ali et al7 and Hussain et al8 (Table 3).
Table 3: Showing incidence of benign and malignant neoplasms.
|
|
Present study |
Ali et al[7] |
Hussain et al[8] |
|
Benign neoplasms |
65% |
74% |
63% |
|
Malignant neoplasms |
35% |
36% |
37% |
Benign tumors were common in fourth decade and malignant tumors in sixth decade and our study observed similar age wise distribution comparable to study done by Hussain et al[8] and Bhavani et al.[9]
Major salivary glands showed high incidence of benign tumors and all the neoplasms of minor salivary glands turned out to be malignant and the present finding was quoted by other study done by Bhavani et al.[9]
The present study saw parotid gland to be the most commonly involved salivary gland followed by submandibular and minor salivary glands. This finding correlates with the studies done by Vergas et al,[10] Hussain et al,[8] Chatterjee et al.[11]
Pleomorphic adenoma was the most reported neoplasm and mixed type histology was common seen in 40% of cases followed by stroma rich (35%) and cellular (25%) rich types. Fabio et al quoted 52.5% of stroma rich, 36.5% of cellular subtype and 21% cases of mixed sutype.[12]However our study is comparable to study done by Bhavani et al[9] who reported mixed type to be most common with 61% followed by 20% of cellular and 19% of stroma rich subtype. (Table 4).
Table 4: Showing histological features in Pleomorphic adenomas.
|
Histopathological type |
Present study |
Fabio et al[12] |
Bhavani et al[9] |
|
Mixed type |
40% |
21% |
61% |
|
Stroma |
35% |
52.5% |
19% |
|
Cellular |
25% |
36.5% |
20% |
Mucoepidermoid carcinoma was the second most common histologic subtype and this is comparable to studies by Soni et al,[13] Spiro et al[14] and Hussian et al.[8]
Warthin tumor seen in 19% of cases showed high incidence in males and was commonly found in parotid. Findings are comparable to study done by Hussain et al[8]and Bashir et al.[15]
Adenoid cystic carcinoma reported in 10% of cases showed minor salivary glands to be the most common site followed by submandibular gland. Similar findings were seen in the study done by Bhavani et al[9]and Rewusuwan et al.[16]Histologically baslaoid cells were found more commonly which is comparable to study done by Bhavani et al[9] and Ellis et al.[17]
Carcinoma ex pleomorphic adenoma was seen in 3% of the cases and showed high grade tumor comparable to studies done by Soni et al.[11]
Adenocarcinoma was reported in 3% of the cases and showed neoplastic glands infiltrating storma.
Conclusion
Despite being rare neoplasms, salivary gland tumors pose challenge to both Pathologist and clinician. The present study concluded that histopathological examination shows diverse overlapping features between various salivary neoplasms and varied subtype among the same neoplasm. Proper diagnosis needs in depth consideration of histological findings to differentiate between benign and malignant neoplasms and grade the malignant neoplasms.
Conflict of Interest: None.
How to cite : N.s S, D.c S, Histopathological spectrum of salivary gland neoplasms. IP J Diagn Pathol Oncol 2019;4(1):54-57
This is an Open Access (OA) journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
![]()
![]()
Viewed: 1691
PDF Downloaded: 702