IP Journal of Diagnostic Pathology and Oncology
Official Publication of Khyati Education and Research Foundation
Official Publication of Khyati Education and Research Foundation
Author Details :
Volume : 4, Issue : 1, Year : 2019
Article Page : 9-15
https://doi.org/10.18231/2581-3706.2019.0002

Abstract
Introduction: Gastric cancer is the 2nd leading cause of cancer mortality worldwide. It has shown to overexpress HER2 and is targetable with trastuzumab. Human epidermal growth factor receptor 2(HER2) is involved in the pathogenesis and poor outcomes of several cancers, including advanced gastric and gastroesophageal junction cancer. According to 2010 large multicentric ToGA study, Trastuzumab based therapy confers overall survival benefit in HER2 positive advanced gastric cancer patients. Hence determining HER2/neu overexpression by immunohistochemistry becomes highly pivotal in identifying the patients who are likely to respond to targeted monoclonal therapy.
Aim and Objectives: Immunohistochemical evaluation of HER2/neu overexpression in gastric carcinomas and its correlation with various clinicopathological parameters.
Materials and Methods: This is a retrospective and prospective study carried out at the Pathology Department of Dr. D.Y.Patil Medical College, Hospital and Research Center, Pimpri, Pune, over a period of 5 years (2012-16). HER2/neu immunohistochemistry (IHC) was performed on all the tumor sections and its overexpression was analysed.
Results: HER2 immunohistochemistry was performed on 50 gastric adenocarcinoma cases, of which 21 cases (42%) showed overexpression. Intestinal subtype showed higher expression rates (48%) compared to diffuse subtype (33%) of gastric cancer and well-differentiated tumors showed highest HER2 [removed]60%).
Conclusion: HER2 overexpression was present in 42% of gastric adenocarcinomas. However, there was no statistical significance between HER2 overexpression and its relation to clinicopathological parameters. It is necessary to conduct further studies with larger samples in order to draw definite conclusions regarding the role of HER2/neu overexpression as an independent prognostic factor.
Keywords: Gastric adenocarcinoma, HER2/neu overexpression, Clinicopathological correlation.
Gastric cancer is the 4th most commonly diagnosed cancer and the 2nd most common cause of cancer related deaths[1]The overall 5 year survival rate of patients with resectable cancer is around 10-30 %.[2]Proximal stomach involvement is more common in western countries and is associated with more aggressive clinical course and a poorer prognosis.[3][4]
In Asian countries, the intestinal subtype of adenocarcinoma is the commonest subtype.[5]Surgical resection is the mainstay of treatment in early stage gastric cancer. However, most patients are diagnosed when the tumor is at an unresectable stage for which chemotherapy becomes the sole treatment option. The survival rate of patients with advanced carcinomas remains poor despite perioperative chemotherapy[6]or chemoradiation.[7]
Staging is an important prognostic factor for gastric carcinoma followed by histological type. However, patients with same stage and histological type may have varied prognosis, hence there is a need to assess additional parameters for better classification, diagnosis and prognosis of the disease.
HER2 is a proto-oncogene encoded by ERBB2 on chromosome 17. It is a transmembrane tyrosine kinase receptor and a member of Epithelial Growth Factor Receptor (EGFR). Its major role is to promote cell proliferation and suppress apoptosis which facilitates uncontrolled cell growth and tumorogenesis. Although HER2 expression was initially associated with breast cancer, it has now been implicated a routine practice in the analysis of advanced gastric cancer as well.[8]
However, immunohistochemical HER2 testing in gastric cancer differs from that of breast cancer because of inherent differences in tumor biology, intra-tumoral heterogeneity of HER2 expression and incomplete membrane staining.[9]
In the 2010 multicentric ToGA study conducted in 122 centers across 24 countries, it was approved that Trastuzumab in combination with chemotherapy can be considered as a new standard option for patients with HER2-positive advanced gastric or gastro-oesophageal junction cancer. Henceforth, the clinical demand for HER2 assessment is rapidly increasing.[10]
Currently, limited data is available for HER2 positivity in gastric carcinomas; various clinical trials for the treatment protocols are underway. There is very little reported data of HER2 expression in gastric cancer in India. Hence this study aims to evaluate HER2/neu status in our patients with gastric carcinoma and its association with clinicopathologic characteristics.
This was a retrospective and prospective unicenter study carried out in Department of Pathology at Dr. D. Y. Patil Medical College, Hospital and Research Centre, from January 2012 to December 2016. The study was approved by the Institutional Ethics committee. A total of 50 diagnosed gastric cancer cases (both gastric biopsy and gastrectomy specimens) who have not received any treatment were included in the study. Clinicopathological parameters, including age, gender, and histological classification was retrieved from the medical records. For prospective study, gastrectomy (total/subtotal) and gastric biopsy specimens were received in 10% buffered formalin while for retrospective study, the slides and paraffin blocks were retrieved from the department of Pathology. Sections (4 ?m thick) were de-paraffinized in xylene and hydrated through a graded series of ethanol. Sections were examined using routine Haematoxylin and eosin stain and classified according to the Lauren’s classification into A) Intestinal and B) Diffuse subtypes.[11]
Immunohistochemical (IHC) staining of HER2 was manually performed on all sections using Thermo scientific c-erB-2/HER-2/neu antibody, with appropriate positive and negative controls.
HER2 scoring was done using scoring scheme proposed by Ruschoff et al.[12]
|
Score |
Surgical specimen staining pattern |
Biopsy specimen staining pattern |
HER-2 overexpression assessment |
|
0 |
No reactivity or membranous reactivity in < 10> |
No reactivity or membranous reactivity in any tumour cell |
Negative |
|
1+ |
Faint/barely perceptible membranous reactivity in >/= 10% of tumour cells; cells are reactive only in part of their membrane |
Tumour cell cluster with a faint/barely perceptible membranous reactivity irrespective of percentage of tumour cells stained |
Negative |
|
2+ |
Weak to moderate complete, basolateral or lateral membranous reactivity in >/=10% of tumour cells |
Tumour cell cluster with a weak to moderate complete, basolateral or lateral membranous reactivity irrespective of percentage of tumour cells stained |
Equivocal |
|
3+ |
Strong,complete, basolateral or lateral membranous reactivity in >/=10% of tumour cells |
Tumour cell cluster with a strong complete, basolateral or lateral membranous reactivity irrespective of percentage of tumour cells stained |
Positive |
Statistical analysis was carried out using the SPSS 20 and Open Epi (version 3) software. P value less than 0.05 were considered statistically significant.
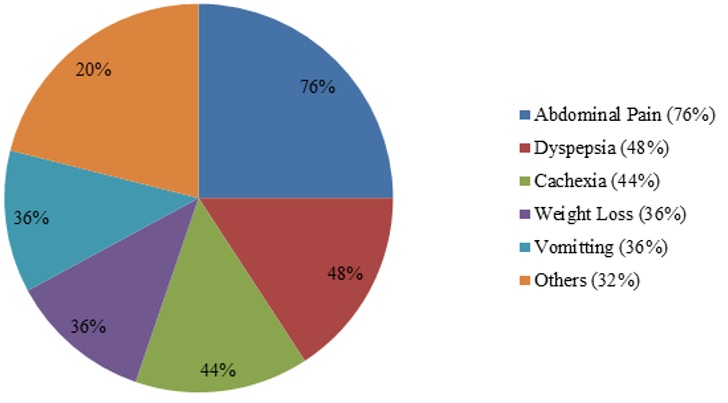
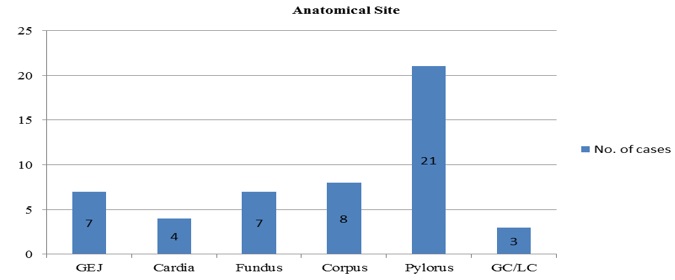
Among the total 50 cases in the present study, there were 13 (26%) gastrectomy specimens while gastric biopsies accounted for 37(74%) cases. Maximum cases were in the 7th decade with the youngest patient being 29 years old while the oldest was 72 years of age. There were 32 (64%) males and 18 (36%) females with an M: F ratio of 1.7:1. Abdominal pain (76%) was the most common complaint followed by dyspepsia (48%) and cachexia (44%), while late stage gastric cancer patients presented with abdominal mass (Fig.1). Pyloric antrum was the most common site followed by gastro-esophageal junction and corpus (Fig. 2).
 |
Click here to view |
Fig. 1: Pie Chart depicting distribution of clinical symptoms
 |
Click here to view |
Fig. 2: Bar graph depicting the site-wise distribution of gastric cancer cases
GEJ-Gastroesophageal junction, GC/LC- Greater curvature/lesser curvature
Table 1: Immunohistochemistry HER2 expression of all cases (n=50):
|
HER2 score |
Gastrectomy specimen |
Gastric Biopsy |
No. of cases |
% positive HER2 |
|
0 |
02 (15%) |
15 (41%) |
17 |
34% |
|
1+ |
03 (23%) |
09 (24%) |
12 |
24% |
|
2+ |
03 (23%) |
07 (19%) |
10 |
20% |
|
3+ |
05 (39%) |
06 (16%) |
11 |
22% |
|
Total |
13 |
37 |
50 |
100% |
Intestinal subtype of gastric carcinoma cases was higher than the diffuse subtype. Poorly differentiated tumours accounted for half of the cases in our study (50%) while well differentiated tumours were the least common (10%).
Other important tumor characteristics such as Intestinal metaplasia, lymph nodal metastasis, muscular infiltration, serosal involvement, vascular invasion, peri-neural involvement and tumoral calcification were also noted in 13 gastrectomy specimens in our study.
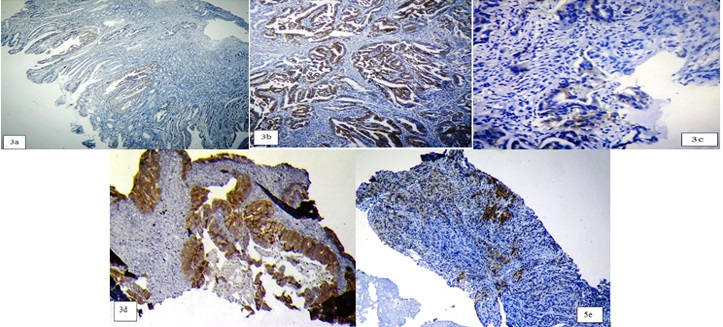
Immunohistochemical study for HER2 in our study revealed 21 cases (42%) with HER2 over[removed]Fig. 3a-3d). Also seen was varying degree of intratumoural heterogeneity for HER2 staining in tumour cells (Fig. 3e). Of the 21 cases with HER2 overexpression, 8 cases were from gastrectomy specimens and 13 cases were of gastric biopsies (Table.1)
100% of the patients with age less than 40 years and more than 70 years showed HER-2 positivity in our study group, while HER-2 positivity in other age groups was less than 50%.
 |
Click here to view |
Fig. 3a: Tumour cells showing HER2/neu score 2+ moderate membranous staining in gastrectomy section, 3b. Score 3+ in gastrectomy section, 3c. Score 2+ in gastric biopsy specimen, 3d. Score 3+ in gastric biopsy specimen, 3e. HER2/neu staining showing intratumoral heterogeneity in gastric biopsy section (IHC, magnification a,d,e x200; b,c x400).
 |
Click here to view |
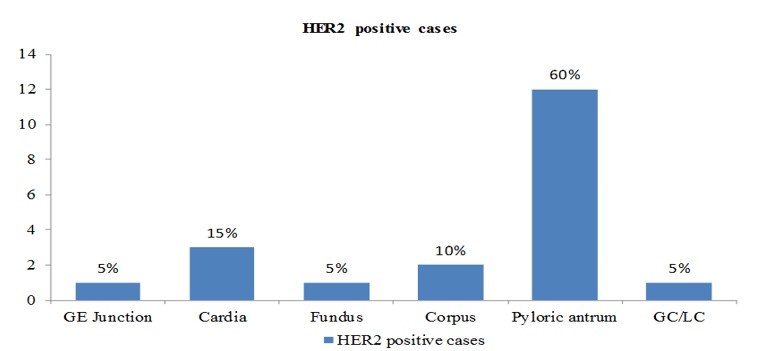
Fig. 4: Bar diagram showing site-wise distribution of HER2/neu positive cases.
Table.2: Analysis of HER2 positivity with Histopathological subtype of gastric cancer:
|
Histopathological Subtype |
No. of patients with HER2 positivity |
% of HER2 positivity |
|
Intestinal (n=29) |
14 |
48% |
|
Diffuse (n=21) |
7 |
33% |
Table.3: Analysis of HER2 positivity according to grading of gastric cancer:
|
Tumor grade |
No. of patients with HER2 positivity |
% of HER2 positivity |
|
Well differentiated (n=5) |
03 |
60% |
|
Moderately differentiated (n=20) |
09 |
45% |
|
Poorly differentiated (n=25) |
09 |
36% |
GEJ-Gastroesophageal junction, GC/LC- Greater curvature/lesser curvature
HER2 over[removed]60%) was seen maximum in the Cardiac region. 50% of cases in the pyloric antrum and corpus showed HER2 overexpression while least HER2 overexpression was noted in the gastro-esophageal junction (Fig. 4).
Regarding HER2 positivity with histopathological subtype of gastric cancer (Table.2), of the 29 cases of Intestinal type of Gastric cancer, 48% (14cases) showed
HER2 positivity; while 33% showed HER2 positivity for Diffuse type (7 cases).
On analysis of HER-2 positivity in relation to grading of gastric cancer, it was observed that HER-2 overexpression for well, moderately and poorly differentiated gastric cancers in our study group was 60%, 45% and 36% respectively. Although well differentiated tumors showed highest HER2 overexpression, the sample size was the smallest of the three groups. There were 9 cases each of HER2 positive moderate and poorly differentiated gastric cancers. (Table.3)
 |
Click here to view |
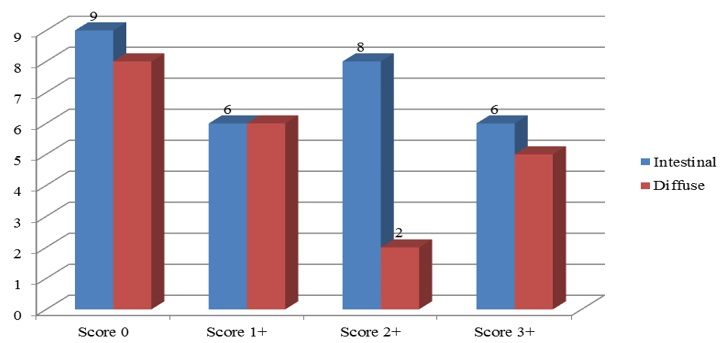
Fig. 5: Bar diagram depicting distribution of HER2 score by type of gastric cancer
Table 4: Relationship between clinicopathological factors and HER2 expression:
|
Clinico-pathological factors |
HER2 positive |
HER2 negative |
p value |
|
Gender |
|
|
0.516 |
|
Male (n=32) |
15 (46.9%) |
17 (53.1%) |
|
|
Female (n=18) |
06 (33.3%) |
12 (66.7%) |
|
|
Age |
|
|
0.646 |
|
<60 n=29)> |
14 (48.2%) |
15 (51.8%) |
|
|
>60 years (n=21) |
07 (33.3%) |
14 (66.7%) |
|
|
Laurens classification |
|
|
0.516 |
|
Intestinal (n=29) |
14 (48.2%) |
15 (51.8%) |
|
|
Diffuse (n=21) |
07 (33.3%) |
14 (66.7%) |
|
|
Tumor Grade |
|
|
0.943 |
|
Well Differentiated (n=5) |
3 (60%) |
2 (40%) |
|
|
Moderately Differentiated (n=20) |
9 (45%) |
11 (55%) |
|
|
Poorly Differentiated (n=25) |
9 (36%) |
16 (64%) |
|
|
Tumor location |
|
|
0.637 |
|
Proximal(GE Junction,Cardia,Fundus,Corpus) (n=23) |
9 (39.1%) |
14 (60.9%) |
Table 5: Comparison of studies showing non-significant p values for HER-2 expression and its correlation to clinicopathological factors:
|
Study |
Age |
Sex |
Location |
Histopathological subtype |
Grading |
|
Sekaran et al 2012(13) |
0.777 |
0.769 |
1.0 |
0.402 |
0.396 |
|
Ali Basi et al 2012(19) |
0.466 |
0.920 |
0.491 |
0.607 |
0.745 |
|
Marx et al 2009(17) |
0.546 |
0.540 |
0.417 |
0.059 |
0.190 |
|
Present study |
0.646 |
0.516 |
0.637 |
0.516 |
0.943 |
The number of cases with HER2/neu score of 0, 1+ and 3+ were almost identical for both the histopathological subtypes; while there were only 2 cases of diffuse subtype with HER2/neu score of 2+ compared to intestinal subtype which had 8 cases (Fig. 5).
Inspite of strong HER2 positivity, there was no statistically significant relationship between HER2 overexpression and clinicopathological factors such as age, gender, tumor site, histological type and tumor differentiation with p values obtained >0.05 (Table.4).
Most gastric cancer patients are diagnosed with advanced disease with the development of distant metastases hence assessment of prognostic markers in these patients should be done.
HER2/neu protein is a transmembrane tyrosine kinase receptor of the epidermal growth factor receptor (EGFR) family which mediates the growth, differentiation and survival of cells. HER2 overexpression results in receptors transmitting excessive cell proliferative signals to the nucleus; thereby directly contributing to the pathogenesis and clinical aggressiveness of the tumor as well as associated with poor prognosis.[13]
Trastuzumab (HerceptinTM) is a monoclonal antibody targeting HER2 protein and has been extensively used in breast cancer with encouraging results.[13] The published data derived from assays employ a variety of polyclonal and monoclonal HER2 antibodies as well as differ in binding affinity, epitope specificity and cross-reactivity with non-HER2 proteins. This may have lead to wide variation in HER2 overexpression ranging from 4-53% as mentioned in a systematic review of 49 studies comprising of 11337 patients[14]. In addition, the possible explanation for the large variability in reported HER2/neu positive rates might |
also be the use of different HER2 antibodies, the different scoring systems being employed, and the skills of the pathologist’s interpretations.[15]
However, Algayer et al reported a 91% rate of HER2 expression in a prospective 203 case study[16]. This may be attributed to the use of highly sensitive streptavidin biotin monoclonal HER2 antibody as well as inclusion of both membranous and cytoplasmic staining.
In this retrospective and prospective study of 50 gastric (13 specimens & 37 biopsies) Adenocarcinoma patients, incidence of HER2 overexpression by immunohistochemistry method and its relationship with clinicopathological features was evaluated. HER2 overexpression considered as IHC score 2+ and 3+ was significantly high (42%); although there was a statistically non-significant relationship with clinicopathological factors (p > 0.05). Sekaran et al in their study with a sample size similar to ours, also showed a non-significant clinicopathological relationship in gastric cancer despite strong HER2 positivity (46%).[13]
In the present study there was no significant correlation between age and HER2 over[removed]p =0.646), although there was 100% HER2 positivity in age groups of <40>70 years. Such varied positivity rates have not been observed in the previous studies; although a non significant relationship with age was observed by Marx et al[17]and Park et al.[18]
There was also a non-significant relationship (p=0.516) between gender and overexpression of HER2 which is in concordance with previous studies conducted by Ali Basi et al[19] who also showed p values of more than 0.05.
According to the results, proximal (39%) and distal (44%) gastric tumors showed similar HER2 overexpression, which is in discordance with a study conducted by Gravalos et al[20] who found higher HER2 positivity in gastro-esophageal junction compared to the stomach. Although there was no statistical correlation between the anatomical site and HER2 over[removed]p=0.637), similar observations were also made by Sekaran et al,[13] Ali Basi et al.[19]
According to Laurens histopathological classification of gastric tumors, Intestinal subtype showed higher HER2 over[removed]58%) compared to the diffuse type (42%) in the present study. Although Kimura et al[21]reported similar findings in their study, there was a significant correlation between HER2 overexpression and the histopathological subtypes which is in discordance with our study (p=0.516).
The cause for intratumoral heterogeneity of HER2 overexpression in gastric cancer is not known, however, it is speculated that this could be merely due to inherent tumour genetic heterogeneity.[15]
There was also no significant relationship between HER2 overexpression and grading of the tumor (p=0.943) (Table 5). Half of the cases of our study were poorly differentiated tumors while well differentiated tumors accounted for the least proportion. Conversely, HER2 overexpression was maximum in well differentiated and the least in poorly differentiated gastric tumors which is in concordance with a study conducted by Raziee et al.[22]
The limitations of the present study are the small number of patients. Various pre and post analytical variables such as intratumor heterogeneity, variation in scoring methods may also have contributed to a statistically non significant relationship. Although the equivocal cases (score 2+) were not subjected to the gold standard method of fluorescent in situ hybridization (FISH), studies have found HER2 overexpression to occur without gene amplification through other transcriptional mechanisms.[13]
As the field of cancer treatment progresses into the era of targeted therapy, pathologists will be faced with increasing demands for tissue biomarker testing. HER2/neu testing for gastric cancer is the first biomarker paving the way for this set of patients. However, this will require continual refinement and analysis of the testing methods for accurate identification of the treatable molecular targets.
Conclusion
Identification and targeted treatment of HER2/neu gastric cancer is the standard method of treatment in many centres. Our study shows 42% HER2 overexpression in gastric adenocarcinoma cases. However, there was no statistical correlation between HER2 overexpression and its clinicopathological parameters. We advocate larger study with long-term follow up in order to accurately identify HER2-positive gastric cancer and to establish the role of HER2 overexpression as an independent prognostic factor.
Conflict of Interest: None.
How to cite : Shah K, Bamanikar S, Pathak P, Wale S C, Bamanikar A, Immunohistochemical testing of HER2/neu protein overexpression in gastric cancer specimens and its clinicopathological correlation. IP J Diagn Pathol Oncol 2019;4(1):9-15
This is an Open Access (OA) journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
![]()
![]()
Viewed: 2165
PDF Downloaded: 566