- Visibility 330 Views
- Downloads 47 Downloads
- Permissions
- DOI 10.18231/j.jdpo.2021.032
-
CrossMark

Abstract
Lingual thyroid (LT) is a developmental defect due to the failure of the thyroid gland to descend to its normal cervical location during embryogenesis. Lingual thyroid has an overall prevalence of 1 in 100,000 to 1in 3,00,000 and is seven to ten times more common in females than in males .Lingual position represents the most frequent ectopic location accounting up to 90% of ectopic cases. It is found at the junction of the anterior two thirds and the posterior third, between the epiglottis and the circumvallate papillae. Most cases are asymptomatic, however, increase in size can cause local symptoms like upper airway obstruction, dysphagia and hemorrhage at any time from infancy to adulthood. Thyroid scintigraphy, neck ultrasound, CT- scan, MRI are some diagnostic modalities that play a vital role in diagnosing ectopic thyroid gland. Treatment of this anomaly includes exogenous L-thyroxine hormone administration, radioiodine ablation therapy and surgery. We hereby report a rare case of lingual thyroid in a young girl reported by fine needle aspiration cytology.
Introduction
Lingual thyroid is a rare anomaly due to aberrant embryogenesis, during the descent of the thyroid gland from the foramen caecum of tongue to its prelaryngeal site in the neck.[1] The prevalence rates vary from 1 in 100,000 to 1in 3,00,000 with females to male ratio ranging from 4:1 to 7:1.[2] Lingual position represents the most frequent ectopic location accounting up to 90% of ectopic cases. [3] Other sites of local thyroid deposition include the cervical lymph nodes, sub mandibular glands and the trachea. [4] The clinical presentation of lingual thyroid varies from asymptomatic to dysphagia, dysphonia, cough, sleep apnoea, stomatolalia, foreign body sensation to obstruction of airway passage and haemorrhage.[5] Even though most of the lingual thyroid glands contain histologically normal tissue; there are reports of carcinoma arising within a lingual thyroid. The diagnosis is based on the clinical features, fine needle aspiration biopsy, laboratory tests and radiographic imaging studies. The rarity of this condition and the paucity of publications in the literature regarding diagnosis by fine needle aspiration cytology prompted us to publish this case.
Case Presentation
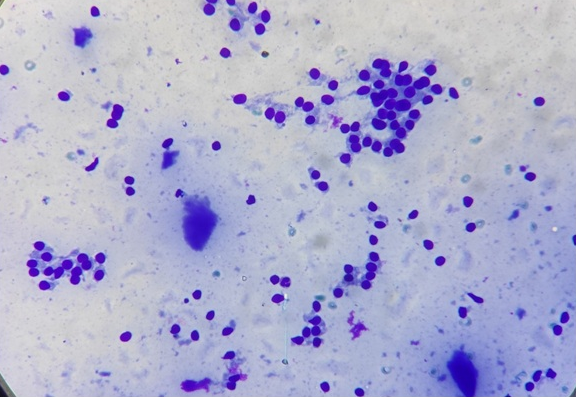
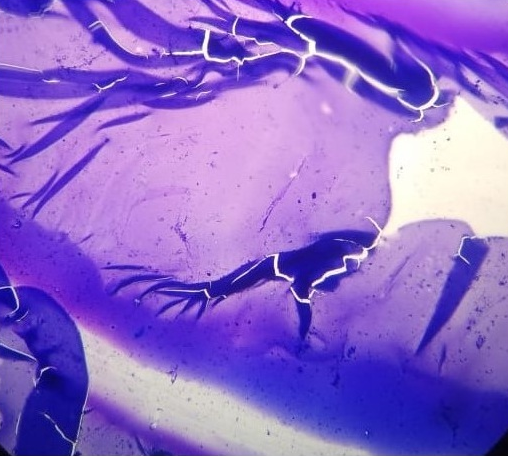
We present a case of 14-year-young girl who presented with complaints of dysphagia and dysphonia since 6 months to our FNAC outdoor department. Her past medical history was insignificant. Her mother denied receiving any medications during pregnancy. On physical examination a smooth, round to oval swelling measuring 2x2cm was noted at the base of the tongue [[Figure 1]]. No signs of bleeding or ulceration was noted. There was no cervical lymphadenopathy. Thyroid function tests revealed euthyroid levels. Other laboratory tests were within normal limits. Thyroid ultrasound scan revealed the absence of thyroid gland in the neck region. Technetium (Tc99m) thyroid scan revealed increased isotope uptake at the base of the tongue and no uptake in the normal thyroid location. On aspirating, a thick mucoid material was obtained which was confirmed to be colloid after staining. Cytology smears revealed benign thyroid follicular cells in clusters with occasional cyst macrophages in a thick colloid background ([Figure 2], [Figure 3]). The diagnosis of lingual thyroid was made on FNAC smears studied. As the patient’s attendant denied any surgical intervention for the mass, she was given thyroid hormone therapy for reduction in size of the gland. Patient is on regular follow-up and is doing fairly well with reduction of the size of the gland as well as her symptoms.

Discussion
The first case of lingual thyroid was reported by Hickman in 1869 on a newborn baby. In lingual thyroid, there is presence of thyroid tissue in the midline at the base of the tongue anywhere between the circumvallate papillae and the epiglottis. It occurs due to failure of descent of normal thyroid tissue from the foramen cecum area of the tongue base, resulting in a midline mass at the base of the tongue.Maternal anti-thyroid thyroid immunoglobulins have been postulated by some authors to be cause of this failure of descent in early fetal life.[6] Besides the normal path of development, ectopic thyroid can be found in mediatinum, heart, esophagus, porta hepatis, ovary etc.[7], [8]
The clinical presentation of lingual thyroid is variable. They mostly present as nodular swelling in the base of the tongue. It is usually seen among adolescents and pregnant women who have an increased demand for thyroid hormones. 33% of patients show hypothyroidism.[8], [9] Further diagnosis of lingual thyroid needs thorough clinical examination, thyroid function tests, ultrasound, CT scan and scintigraphy. Technetium-99, Iodine-121 or I-131 are used in scintigraphy which detect ectopic thyroid tissue and show absence or presence of normally positioned thyroid tissue.
Asymptomatic cases need regular follow-up. Levothyroxine replacement therapy is effective in mild symptomatic cases. In conditions like airway obstruction or complications due to mass effect, surgery is the preferred method of management after consideration of patient’s age, functional thyroid status and complications of the swelling.[10] Several surgical routes are used like transoral, transhyoid, suprahyoid and lateral pharungotomy. The transoral route is preferred as it avoids lingual nerve injury and deep cervical infections.[9], [10] Despite being benign in majority of cases there are reports of carcinoma arising within a lingual thyroid. So, early diagnosis and treatment of lingual thyroid is essential with regular follow-up.[10] FNAC is thus an inexpensive tool to exclude the rare possibility of malignancy in such cases.
Conclusion
Lingual thyroid is a rare developmental anomaly. It should be considered in the differential diagnosis of tongue masses in children and adolescents that includes lymphangioma, minor salivary gland tumours, midline branchial cyst, thyroglossal duct cyst, epidermoid cyst and lipoma. Thorough clinical examination, neck imaging by ultrasound or CTscan and FNAC can help in clinching the correct diagnosis. Early diagnosis and appropriate management can help to manage the condition and prevent complications in these cases.
Source of Funding
No financial support was received for the work within this manuscript.
Conflicts of Interest
There are no conflicts of interest.
References
- Batsakis J, El-Naggar A, Luna M. Pathology Consultation Thyroid Gland Ectopias. Ann Otol Rhinol Laryngol . 1996;105(12):996-1000. [Google Scholar] [Crossref]
- Ross D, Mcqueen D, Kettles H. Land rehabilitation under pasture on volcanic parent materials - Changes in soil microbial biomass and C-metabolism and N-metabolism. Soil Res. 1994;32(6). [Google Scholar] [Crossref]
- Basaria S, Westra W, Cooper D. Ectopic Lingual Thyroid Masquerading as Thyroid Cancer Metastases. J Clin Endocrinol Metab. 2001;86(1):392-39. [Google Scholar] [Crossref]
- Babazade F, Mortazavi H, Jalalian H, Shahvali E. Thyroid tissue as a submandibular mass: a case report. J Oral Sci. 2009;51(4):655-7. [Google Scholar] [Crossref]
- Chawla M, Kumar R, Malhotra A. Dual Ectopic Thyroid: Case Series and Review of the Literature. Clin Nuclear Med. 2007;32(1):1-5. [Google Scholar] [Crossref]
- Felice M, Lauro R. Thyroid Development and Its Disorders: Genetics and Molecular Mechanisms. Endocr Rev. 2004;25(5):722-46. [Google Scholar] [Crossref]
- Ferlito A, Giarelli L, Silvestri F. Intratracheal thyroid. J Laryngol Otol. 1988;102(1):95-6. [Google Scholar] [Crossref]
- Arriaga M, Myers E. Ectopic Thyroid in the Retroesophageal Superior Mediastinum. Otolaryngol–Head Neck Surg. 1988;99:338-40. [Google Scholar] [Crossref]
- Felice MD, Lauro RD. Thyroid Development and Its Disorders: Genetics and Molecular Mechanisms. Endocr Rev. 2004;25(5):722-46. [Google Scholar] [Crossref]
- Zitsman J, Lala V, Rao P. Combined cervical and intraoral approach to lingual thyroid: A case report. Head Neck. 1998;20(1):79-82. [Google Scholar] [Crossref]