- Visibility 67 Views
- Downloads 17 Downloads
- Permissions
- DOI 10.18231/j.jdpo.2021.009
-
CrossMark

Abstract
Introduction: Over the years, nature has witnessed the occurrence of pandemics caused by influenza viruses of different strains due to their unique capability of antigenic variations and aggressive behavior. This study aims to understand and document the general characteristics and biochemical findings of Influenza A H1N1 infection.
Materials and Methods: This study revolved around hundred patients presenting with influenza like illness. The general, clinical and relevant laboratory investigation findings of Influenza A H1N1 positive patients were studied and documented
Results: Out of hundred patients with influenza like illness, sixty-five positive patients were studied excluding the thirty-five negative patients. The age range of the patients was wide from 1 month to 75 years, with seven cases having had comorbid conditions and six cases with history of exposure. Fever was the most common symptom in all cases, followed by cough, sore throat, nasal catarrh, difficulty in breathing and vomiting. Fourteen patients took liver function tests among whom eight showed elevation of enzymes and two out of twenty-one tested had hypokalemia.
Conclusion: The unpredictable nature, varied clinical and laboratory expressions of the disease make it essential to study and understand the various characteristics of the Influenza A H1N1 infection
Introduction
The year 2009 saw the unfolding of a unique strain, of a virus named Influenza A H1N1, with the first cases being reported from Mexico in March. In a span of three months it was declared a pandemic by the WHO.[1]
With a distinct combination of gene segments from swine, avian and human lineages, this new virus, with a strain different from that seen in the past, overcame the complex species barrier to infect humans, leading to influenza-like symptoms and progressing in a few cases to viral pneumonia, respiratory failure, multiple organ failure and death. [2]
The occurrence of the 2009 H1N1 virus is an unparalled event in modern virology as it neither fits the classic definition of a new subtype nor drift with no previous infection experience and without direct evolutionary relationship with the recently circulating H1N1 viruses of human origin. [3]
The clinical course being mostly benign with symptoms being mild and subclinical, Pneumonia, is the most common and important complication. [1] Rate of illness, hospitalization and death have varied widely according to country. Diffuse viral pneumonitis associated with severe hypoxemia, ARDS, and sometimes shock and renal failure are the frequent reasons for hospitalization and intensive care. [4]
Influenza-like illness (ILI) is defined by the CDC as fever (temperature ≥100°F or 37.8°C) and either cough or sore throat in the absence of another known cause. A confirmed case of 2009 H1N1 infection is defined by ILI with positive test results for the 2009 H1N1 virus by either real-time reverse transcriptase polymerase chain reaction (rRT- PCR) or viral culture. A probable case is ILI with positive influenza A test results but negative results for seasonal H1 and H3 by rRT-PCR. A suspected case does not meet either definition but is either a person younger than 65 years hospitalized for ILI or a person of any age with ILI and an epidemiological link to a confirmed or probable case within 7 days of illness onset. The 2009 H1N1 influenza can be contracted through 3 routes: contact exposure (when a contaminated hand is exposed to facial membranes), droplet spray exposure (when infectious droplets are projected onto mucous membranes), and airborne exposure (via inhalation of infectious airborne particles). [3]
Materials and Methods
One hundred patients, admitted to hospitals attached to JJM Medical College Davangere, presenting with Influenza like illness were tested for Influenza A H1N1 by Rapid SD BIOLINE influenza antigen test kit in clinically directed cases and by rRT-PCR, in category C patients using throat swab, sent to department of Virology, NIMHANS, Bangalore through the DSO. Patients who took rapid screening test were all negative. rRT PCR proved cases were included in the study. Out of hundred patients, sixty five were positive and thirty five were negative. In this study general, clinical characteristics and relevant laboratory investigation findings of rRT-PCR tested, positive, patients were studied and documented.
Biochemical tests-LFT and serum electrolytes were done at the discretion of clinician by automated analyser COBAS Integra 400 Roche, Germany using standardized protocols as per the manufacturers instruction. Blood and sputum culture were done at the discretion of clinician in the department of microbiology
Results
This study was done during July 2009 to June 2011.From the hundred patients with influenza like illness, sixty five patients proven to be positive for Influenza A H1N1 via rRT-PCR test were included and the rRT-PCR negative thirty five patients were excluded.
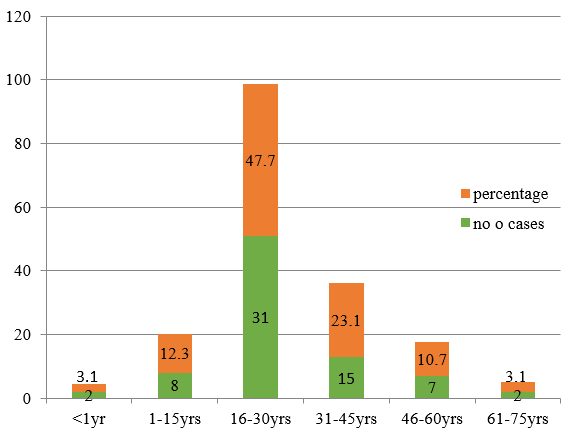
Patients studied were aged from 1month to 72 years with average age being 29.73 yrs. 47.7% of the patients were in the age range of 16-30yrs followed by 15 (23.1%) patients in age cluster of 31-45years ([Figure 1])
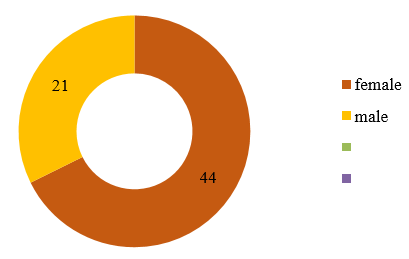
Majority of the patients were females 44 (67.7%) followed by 21 (32.3%) of males ([Figure 2] )
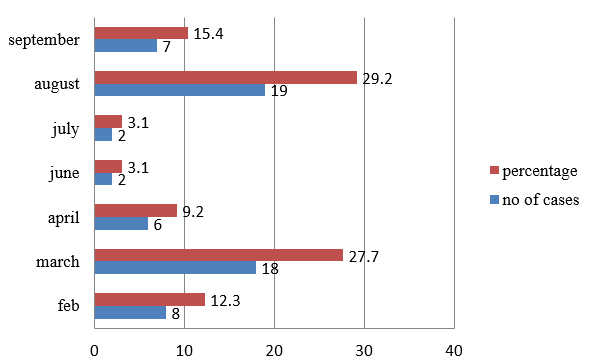
Majority of the cases occurred in the months of March and August.14 cases occurred in the year 2009, 47 cases in the year 2010 and two cases in the year 2011.([Figure 3])
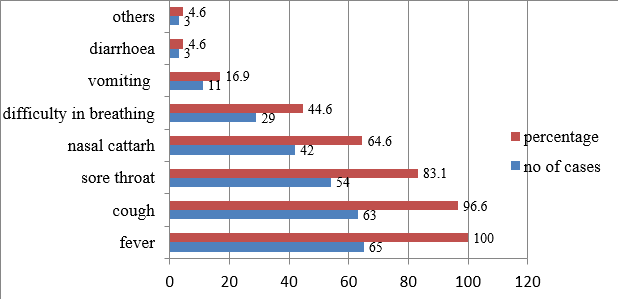
All sixty five patients had fever, while the least common symptoms were headache and irritability seen in 2 and 1 patient respectively. Second most common symptom was cough seen in 63 cases followed by sore throat (54), nasal catarrh (42), difficulty in breathing (29), diarrhea (11) and vomiting (3)([Figure 4])
Out of sixty five cases, seven cases had co existing conditions, two cases of asthma, three cases of diabetes mellitus, one case of diabetes mellitus with hypertension and one case was a case of third trimester pregnancy.([Table 1])
|
Co existing condition |
Number of cases |
|
Diabetes mellitus |
4 |
|
Asthma |
2 |
|
Hypertension |
1 |
|
Pregnancy |
1 |
Out of sixty-five cases, six cases had history of exposure, among them one had a history of air travel, two had history of contact with confirmed case of influenza A H1N1 and two had history of contact with suspected case of influenza A H1N1.
Out of the fourteen tested for LFT, three cases showed elevated SGOT/AST levels, four patients showed elevated SGPT /ALT levels and one showed elevated ALP levels.([Table 2])
Serum sodium and serum potassium estimation was done in 21 patients. Two cases showed hypokalemia.
|
Parameter |
Normal |
Range of our observation |
|
Total bilirubin (mg/dl) |
0.3 – 1.0 |
0.2-0.8 |
|
Direct bilirubin (mg/dl) |
0.1 – 0.3 |
0.1-0.2 |
|
Indirect bilirubin (mg/dl) |
0.2– 0.7 |
0.1-0.6 |
|
Total protein (gm/dl) |
6 – 8.3 |
5.8-7.4 |
|
Albumin (gm/dl) |
3.5 – 4.5 |
3.4-3.8 |
|
Globulin (gm/dl) |
2.5 – 3.8 |
2.9-3.6 |
|
SGOT/AST (IU/L) |
10 – 37 |
25-70 |
|
SGPT/ALT (IU/L) |
5 – 4 |
26-56 |
|
ALP (IU/L) |
Upto125 |
48-154 |
Blood culture was done in 10 cases and all were negative. Sputum culture was done in six patients, with none of the cases showing pathognomonic isolation. In one case endotracheal aspirate culture was done. Isolation of klebshiella and candida species was achieved.
Discussion
Most of the cases were young adults and middle aged in the age range of sixteen to forty five years, amounting to (70.8%), similar to studies by Mu YP et al, [2] Jain S et al,[5] Ong AK et al[6] and Duque V et al.[7]
Similar to patients in study done by Duque et al7 and Ong et al,[6] the frequency of symptoms was fever, cough, sore throat, nasal catarrh, breathlessness, vomiting and diarrhea in that order in our study as well. Whereas cough was the most common symptom followed by fever, sore throat, nasal catarrh, breathlessness and vomiting in Chudasama et al[8] study.
Like seasonal influenza, a great majority of cases have fever, cough, sore throat and runny nose. What is critically important, however, is that in a small proportion of patients, the clinical course tends to deteriorate rapidly, leading to complications and death.[2]
Coexisting conditions like diabetes and cardiovascular, neurologic, and pulmonary diseases, including asthma have been reported in patients, hospitalized with influenza like illness.[9]
The coexisting conditions seen in patients in our study were low in number, which were diabetes mellitus (4), asthma (2) and pregnancy (1) similar to study done by Chudasama et al,[8] out of two seventy four cases ninety cases had comorbid illness. Diabetes was seen in twenty cases, fifteen cases had chronic pulmonary diseases and fifteen cases were pregnant.
The extent to which these comorbidities contribute to severity of disease is unclear because a large portion of the aboriginal population (which may be a risk factor itself on the basis of genetic susceptibility) often have such comorbidities.[10]
In Singapore Chan et al[11] noted that out of thirty one H1N1 cases thirty cases had history of foreign travel and twenty seven patients had history of close contact with a suspected case, while in our study out of sixty five cases only one case had history of foreign travel and five cases had contact history.
The infectious particles of the H1N1 virus are estimated to be less than 10 mm in size and normal room air currents can keep them airborne for long periods of time. These particles are easily spread unless adequate protection and control are provided.[6]
In our study out of the 65 cases, 13 (20%) died of the disease. In a study done by Jain S et al[5] death was seen in (7%) out of 272. The median age was 27 yrs. The median age of the cases in our study was 41yrs. Out of the 13 cases 4 cases had underlying medical condition while in study by Jain et al 13 of the 19 cases had underlying medical condition.
In our study eight out of fourteen patients showed alterations in liver enzymes. SGOT, SGPT and Alkaline phosphatase levels were elevated in 3/14(21.4%) cases, 4/14(29%) and 1/14(7%) cases in comparison to 9/225(4%), 17/225(8%) and 5/225(2.2%) cases respectively in study done by Mu YP et al.[2] Bilirubuin and protein values were within normal limits.
Hypokalemia was seen in two cases when compared to 88/225 cases in study done by Cao B et al[12] in China.
Conclusion
The clinical manifestations of influenza A H1N1 virus infection range from self- limited uncomplicated sub febrile respiratory illness to severe and even fatal respiratory disease and extrapulmonary disease. Gastrointestinal symptoms include vomiting, diarrhea and abdominal pain.
Since Influenza A H1N1 is unpredictable in its presentation, etiological diagnosis based on clinical presentation may be difficult. H1N1 infection should be considered in the differential diagnosis for patients presenting with fever, cough, sore throat, nasal catarrh, difficulty in breathing or pneumonia
Source of Funding
No financial support was received for the work within this manuscript.
Conflict of Interest
The authors declare that they have no conflict of interest.
References
- Bewick T, Myles P, Greenwood S, Nguyen-Van-Tam JS, Brett SJ, Semple MG. Clinical and laboratory features distinguishing pandemic H1N1 influenza-related pneumonia from interpandemic community-acquired pneumonia in adults. Thorax. 2011;66(3):247-52. [Google Scholar] [Crossref]
- Mu YP, Zhang ZY, Chen XR, Xi XH, Lu YF, Tang YW. Clinical features, treatments and prognosis of the initial cases of pandemic influenza H1N1 2009 virus infection in Shanghai China. Q J Med . 2010;103(5):311-7. [Google Scholar] [Crossref]
- Sullivan S, Jacobson RM, Dowdle WR, Poland GA. 2009 H1N1 Influenza. Mayo Clin Proce. 2010;85(1):64-6. [Google Scholar] [Crossref]
- Hayden FG. Clinical Aspects of Pandemic 2009 Influenza A (H1N1) Virus Infection. N Engl J Med. 2010;362:1708-19. [Google Scholar]
- Jain S, Kamimoto L, Bramley A, Schmitz A, Benoit S, Sugerman D. Hospitalized Patients with 2009 H1N1 Influenza in the United States, April–June 2009. N Engl J Med. 2009;361(20):1935-44. [Google Scholar] [Crossref]
- Ong AK, Chen MI, Lin L, Tan AS, Nwe NW, Barkham T. Improving the clinical diagnosis of influenza--a comparative analysis of new influenza A (H1N1) cases. PLoS One. 2009;4. [Google Scholar]
- Duque V, Cordeiro E, Mota V, Vaz J, Morais C, Rodrigues F. The early days of pandemic (H1N1) 2009 virus infection in the central region of Portugal. Rev Port Pneumol. 2010;16(6):870-9. [Google Scholar] [Crossref]
- Chudasama RK, Patel UV, Verma PB, Amin CD, Savaria D, Ninama R. Clinico-epidemiological features of the hospitalized patients with 2009 pandemic influenza A (H1N1) virus infection in Saurashtra region. Lung India. 2009;28(1):11-6. [Google Scholar]
- . Inactivated influenza vaccine.What you need to know 2010-2011. . . [Google Scholar]
- Gill J, Sheng Z, Ely S, Guinee D, Beasley M, Suh J. Pulmonary Pathologic Findings of Fatal 2009 Pandemic Influenza A/H1N1 Viral Infections. Arch Pathol Lab Med. 2010;134(2):235-43. [Google Scholar] [Crossref]
- Chan WL, Goh HK, Vasu A, Lim BL, Seow E. Experience of a screening centre for influenza A/H1N1: the first 50 days. Emerg Med J. 2011;28(1):18-24. [Google Scholar] [Crossref]
- Cao B, Li XW, Mao Y, Wang J, Lu HZ, Chen YS. Clinical features of the initial cases of 2009 pandemic influenza A (H1N1) virus infection in China. N Engl J Med. 2009;361(26):2507-17. [Google Scholar]